
|
|
Introduction - case 1618
|
|





First examination (1st row of images)
Clinical presentation. A 51-year-old woman was referred for aspiration cytology of a thyroid nodule. She was examined because of depression and weight gain. (We met the patient in May 2020 during the COVID epidemic. Her endocrinologist did not meet the patient.)
Palpation: no abnormality.
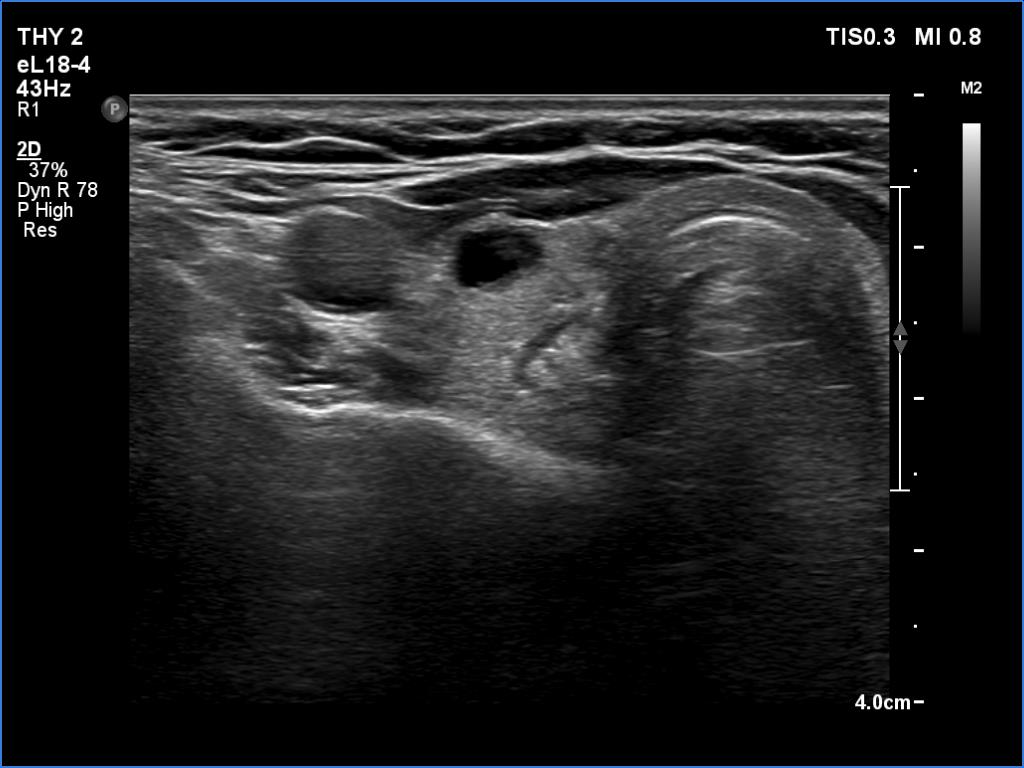
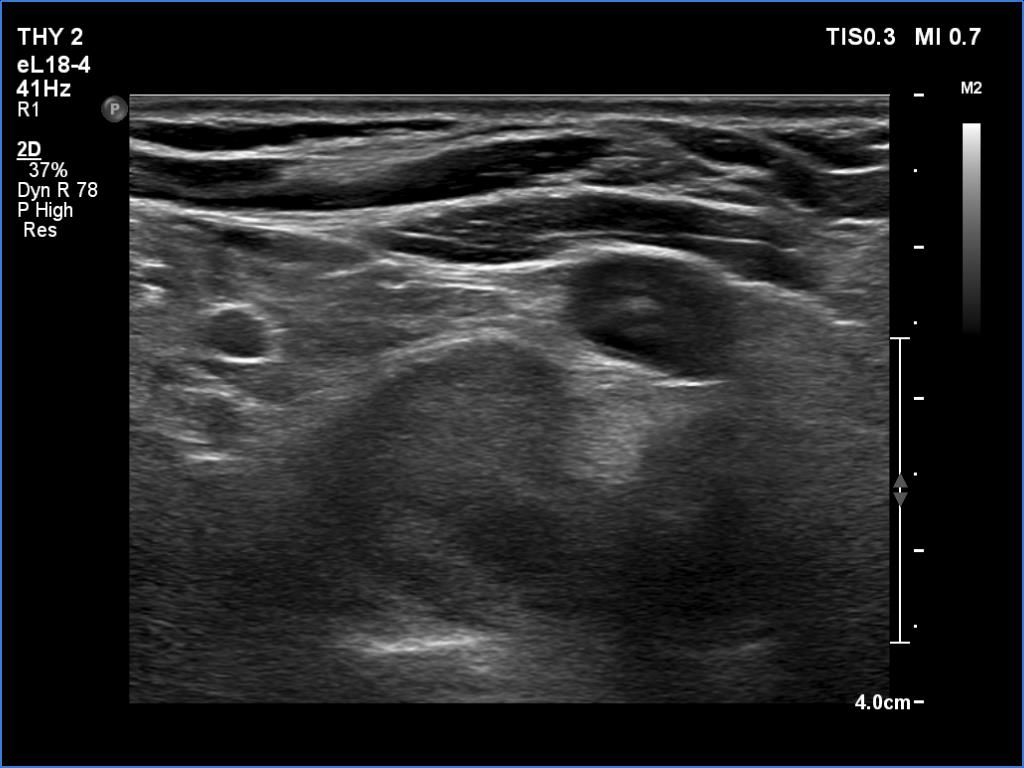
Ultrasonography. The thyroid was echonormal and had several tiny hypoechoic areas and an echonormal nodule in the lower third of the right lobe. We did not find any lesion of clinical or oncological significance.
Second examination 6 month later (2nd row of images)
Clinical presentation. The patient was referred for evaluation of hyperparathyroidism. Elevated calcium and parathyroid hormone levels were found during the first evaluation. (These findings were not yet available when I first examined the patient.) Further evaluation disclosed a hyperfunctioning right lower parathyroid. The patient was operated on but no parathyroid tissue was found on histopathology. (A more experienced parathyroid surgeon was quarantined at the scheduled time of the operation, so a less experienced colleague performed the surgery.) Both hypercalcemia and hyperparathyroidism have persisted.
Palpation: no abnormality.
Laboratory tests: parathormone 129 pg/mL (normal value: 12-88), serum calcium 2.89 mM/L, phosphate 0.71 mM/L.
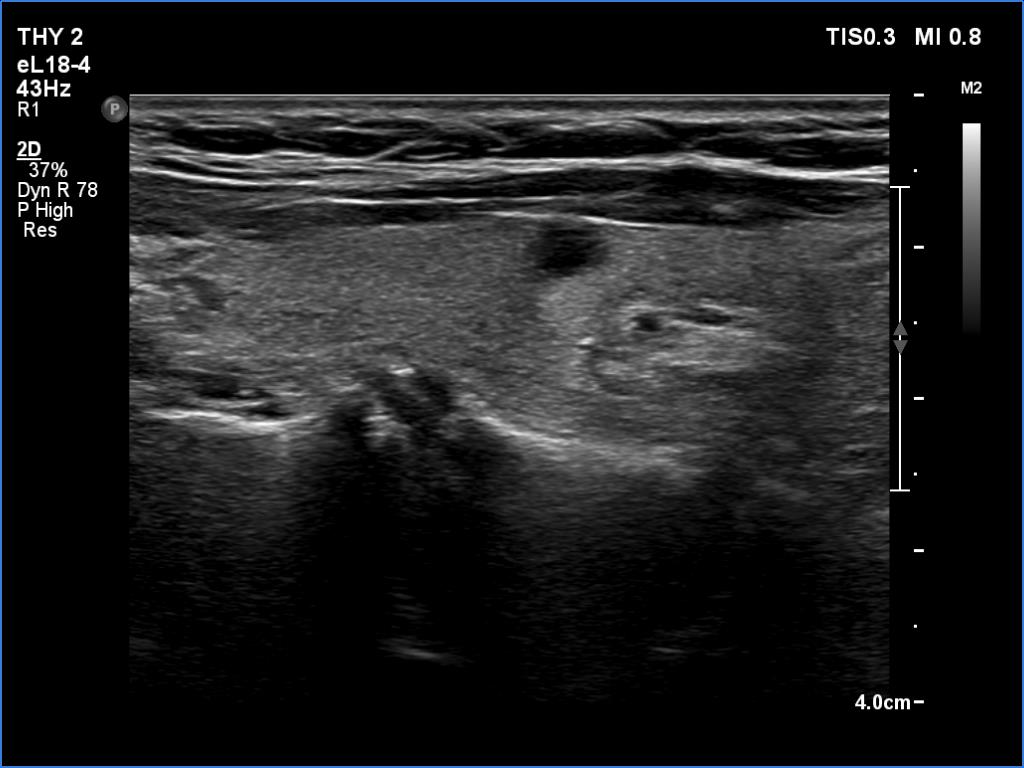
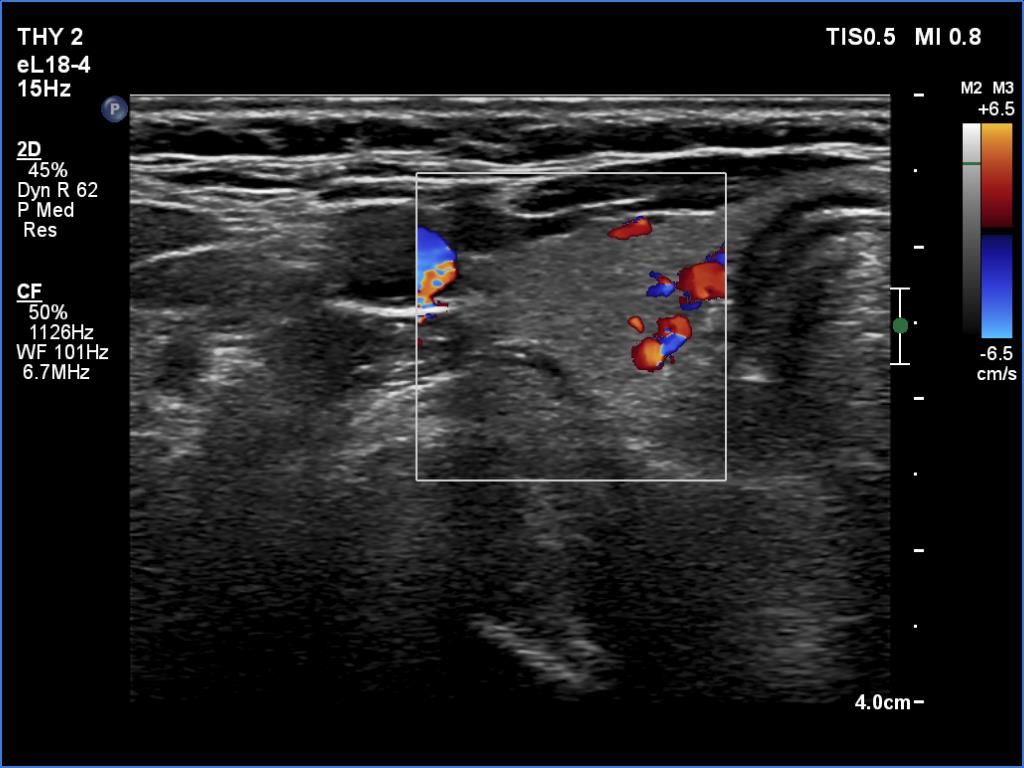
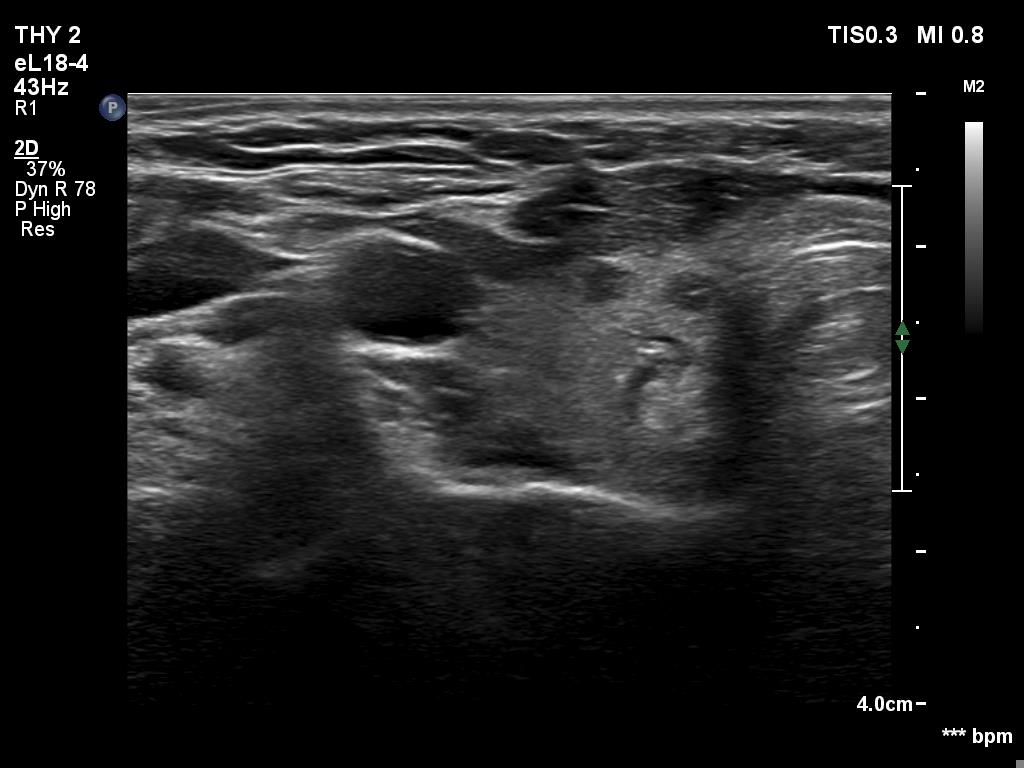
Ultrasonography revealed a hypoechoic mass corresponding to the right lower parathyroid.
Cytology resulted in benign lesion, a pattern which corresponded to a parathyroid adenoma.
The patient was reoperated and histopathology disclosed a parathyroid adenoma according to the right lower parathyroid.
Comment. Reviewing the study, several failures and unfortunate circumstances can be revealed.
-
If we compare the first and second ultrasound examination, it is evident that the ultrasound examination was not performed according to the rules of the profession at the first visit. (I will just mention that although in this case we only videotaped part of the entire study, we obviously overlooked the parathyroid gland under the right lobe. The reason for this is that we did not examine the part below the thyroid in the transverse section, and in the longitudinal section we started to examine the lower part of the thyroid too medially.)
-
I have to confess, that this is not the only missed parathyroid adenoma in my practice, in addition to this was the largest among them. Normally, if a high level of calcium or parathyroid hormone is revealed after an ultrasound examination, the patient is re-examined. This was not initiated by the patient's endocrinologist due to the situation caused by the COVID-19 epidemic.
-
Parathyroid surgery requires a lot of practice. The less experienced colleague who undertook the surgery judged that he would find a 1.5-centimeter lesion. But he also failed.