
|
|
Intranodular hyperechogenic figures - case 1158
|
|







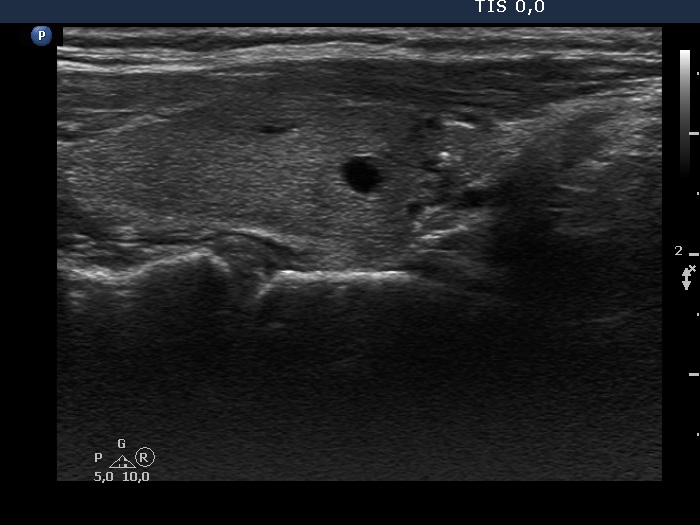





First examination (first row of images):
Clinical presentation: A 52-year-old woman was referred for ethanol sclerotherapy. Her cystic nodule was three times drawn off but recurred within weeks and caused compression signs. Cytology resulted in non-diagnostic, cystic degeneration.
Palpation: an elastic nodule in the isthmus.
Functional state: euthyroidism with TSH 1.76 mIU/L.
Ultrasonography. The thyroid was echonormal. There were several small cystic areas in the right lobe, while there was a large cyst in the isthmus. The latter lesion contained small, moderately hypoechogenic solid part which separated a small cystic area from the larger one. The solid portion contained smaller non-specific, and bit larger and brighter hyperechogenic granules. These are equivocal figures, the presence of microcalcifications cannot be excluded.
We told the patient that the possibility of a papillary carcinoma cannot be excluded on ultrasound presentation even if the cytology would be benign. Surgery was advised.
An isthmusectomy was performed. Histopathology disclosed benign hyperplastic nodule.
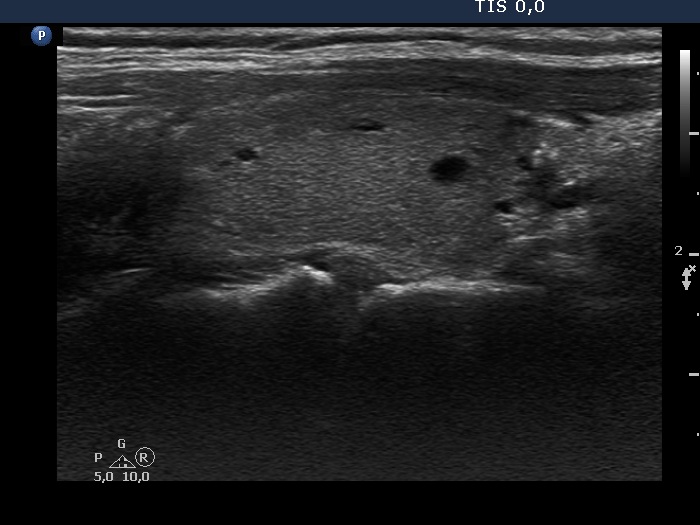
Second examination 9 months after surgery (second row of images):
Clinical presentation: The patient had no complaints.
Palpation: no abnormality.
Ultrasonography: The right and the left lobe remained unchanged except for the appearance of a moderately hypoechogenic lesion in the lower, isthmic part of the right lobe. This lesion contained various hyperechogenic granules and was avascular on Doppler mode. The ultrasound presentation stood for a granulation around surgical thread.
Comments.
-
We perform sclerotherapy even if the cytology is non-diagnostic if the ultrasound presentation is calming. Vice versa, we did not perform sclerotherapy of a cystic nodule in the event of benign cytology if the ultrasound presentation is suspicious.
-
The lesion which has appeared on post operative ultrasound might be a regenerative tissue or a granulation around surgical thread. The latter is more likely because the former usually disappears within 4 months after the operation.