
|
|
Intranodular hyperechogenic figures - case 951
|
|




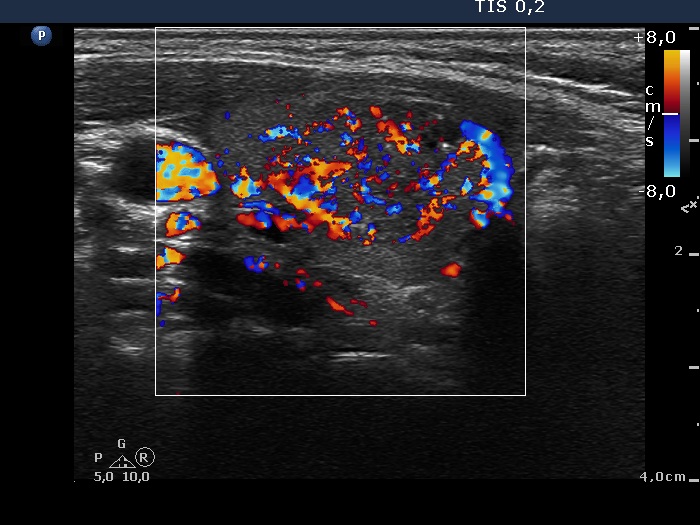





First examination (first row of images):
Clinical presentation: A 30-year-old woman noticed a lump in the right lobe one week ago.
Palpation: a not firm nodule in the right lobe.
Functional state: euthyroidism with TSH 0.83 mIU/L, FT4 14.1 pM/L.
Ultrasonography. The thyroid was echonormal. There were two nodules in the right lobe, the upper one was echonormal-cystic presenting halo sign and perinodular blood flow. It seemed a peripheral-type cyst. The lower was a suspicious nodule: this was hypoechogenic, had a blurred border and lobulated margins and showed an irregularly increased vascularization. At first sight, this nodule contained numerous microcalcifications. However, these bright echogenic figures were partly related to dorsal cystic areas and some of them had a short tail. Therefore, beside microcalcifications, back wall figures and comet tail artifacts had to be aslo considered.
3.5 mL brown fluid was aspirated form the upper nodule, and cytology resulted in cystic degeneration. There were only a few cells on the smear gained from the lower lesion and cytology resulted in non-diagnostic report.
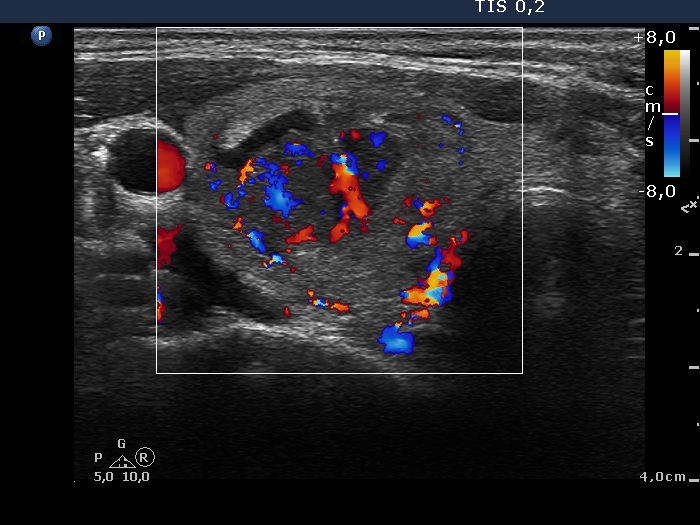
Follow-up examination 2 months later (second row of images):
Clinical presentation: The patient had no complaints.
Palpation: a firm nodule in the right lobe.
Ultrasonography: The pattern was basically unchanged. However, it became clear that the upper cystic nodule is in fact a central-type cyst.
Cytology of the suspicious nodule was again not diagnostic.
Suggestion: surgery.
A right lobectomy was performed, and histopathology disclosed benign hyperplastic nodules.
Comments.
-
It is worth thoroughly and repeatedly analyze the lesion in the right lobe which was lower to the larger nodule. The issue is the presence of microcalcifications. Thorough analysis of these that these partly belong to back wall figures, partly to comet-tail artifacts. (It is worth comparing the bright hyperechogenic figures also present in the larger cystic nodule with those found in the lower lesion.) Nevertheless, the presence of microcalcifications cannot be ruled out.
-
In the event of a non-diagnostic puncture, we repeat the cytology after at least 4 weeks. We have found a higher repeatedly non-diagnostic rate if we repeat the aspiration within 2 weeks compared with a reaspiration at least 4 weeks after the first attempt.