
|
|
Halo sign and vascular pattern of nodules - case 2249
|
|




First examination (first row of images)
Clinical data: A 21-year-old woman was referred for evaluation on a nodular goiter. She has noticed an enlargement in the left lobe for a year. On evaluation in another institute, a cystic nodule was diagnosed with a 26 mm maximal diameter and 3 mL brown fluid was aspirated. Cytology resulted in benign cystic lesion.
Palpation: The right lobe was suspicious having a nodule.
Laboratory test: TSH 2.21 mIU/L.
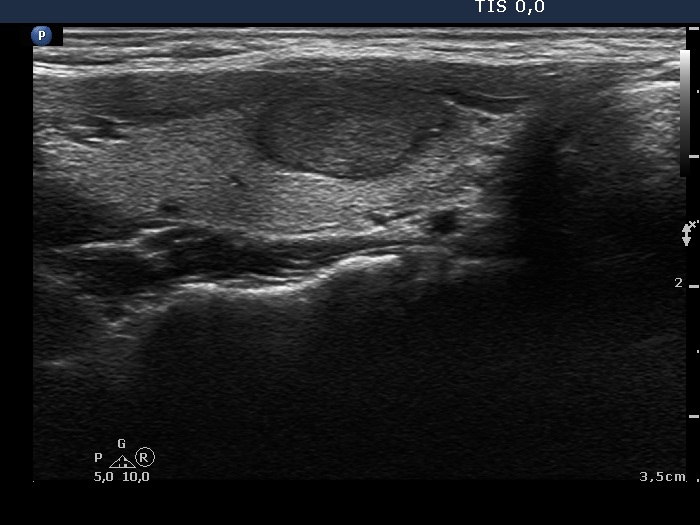
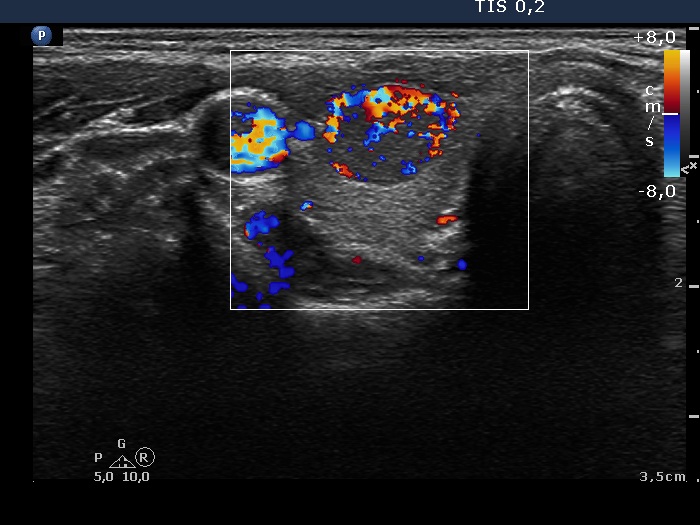
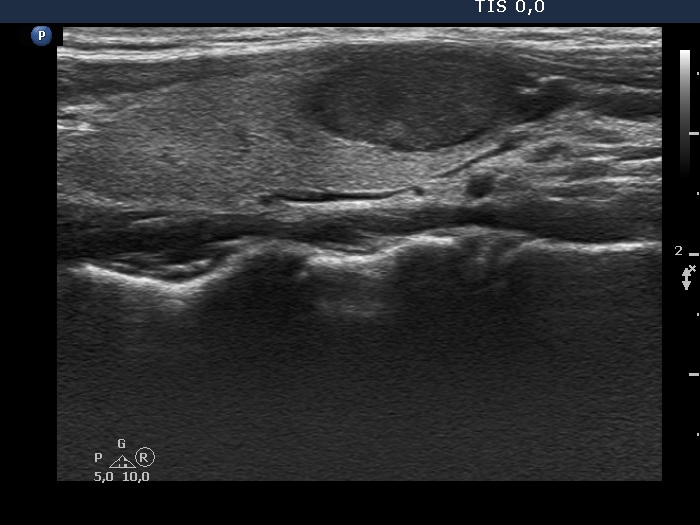
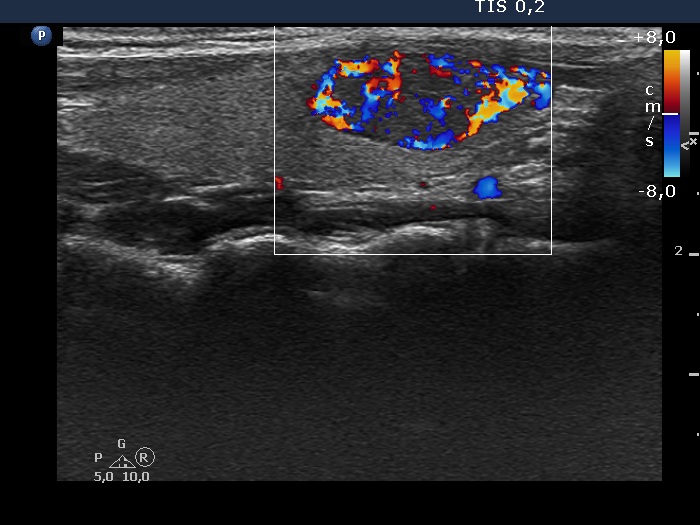
Ultrasonography. The thyroid was echonormal and presented a moderately hypoechoic nodule in the right lobe and a cystic nodule with minimally hypoechoic solid part corresponding to the previously aspirated cystic lesion. The largest diameter of the latter was 11 mm which means that cyst has not refilled. The nodule in the right lobe showed irregular, more hypoechoic areas all along at the periphery. This pattern mimicked halo sign, but indeed the lesion did not have a real halo. The vascularization of the nodule in the right lobe presented an irregularly increased intranodular blood flow while the lesion in the left lobe did signs of perinodular vascularization.
Cytology was performed form the lesion in the right lobe and resulted in follicular proliferation.
Combined ultrasound-cytological diagnosis was benign follicular proliferation.
Suggestion: ultrasound in a year.
Second examination 3 years later (second row of images)
Clinical data: The patient had no complaints.
Palpation: unchanged.
Laboratory test: TSH 0.79 mIU/L.
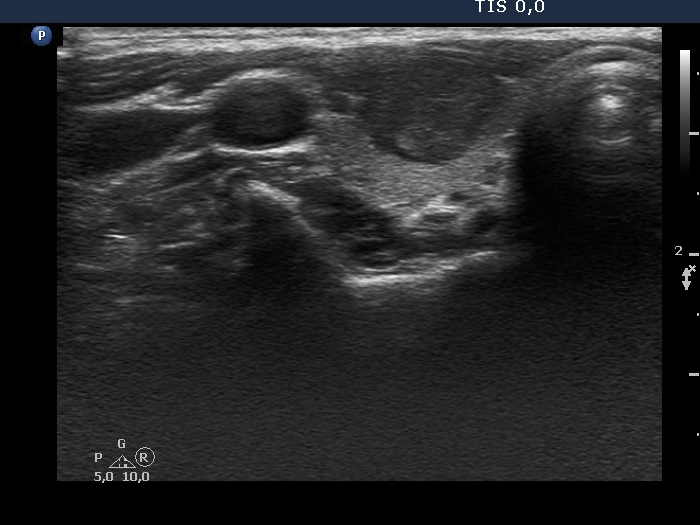
Ultrasonography. Both the pattern and the size of the nodule in the right lobe remained unchanged. The cystic content of the left lobule has disappeared, it was replaced by inhomogeneous solid part. The vascularization of this lesion has also changed, the intranodular vascularization has become significantly increased.
Suggestion ultrasound in three years.
Comment. In the event of a cytological pattern which raises the suspicion of follicular tumor, we review the ultrasound records. By definition, a follicular tumor is surrounded with capsule. If none of the ultrasound signs of a capsule can be found, i.e. the nodule has neither halo nor perinodular blood flow than the risk of a follicular tumor is surely less than 5%. Be aware that more than 25% of cytologically suspected follicular tumors prove to be hyperplastic nodules on histopathology.