
|
|
Case 116
|
|








Clinical presentation: A 51-year-old woman was referred for an evaluation of hypothyroidism detected on routine examination.
Palpation: Both lobes were firm, but no nodule was palpable.
Laboratory evaluation: TSH 22.7 mIU/L, FT4 6.9 pM/L.
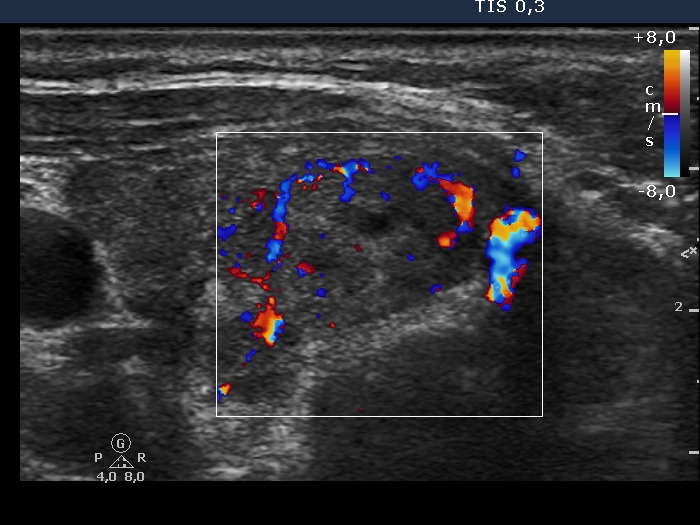
Ultrasonography. The thyroid was moderately hypoechogenic. There were numerous hyperechogenic areas within. A larger, more hypoechogenic lesion was found in the lower pole of the right lobe. The lesion did not show halo sign but had perinodular blood flow.
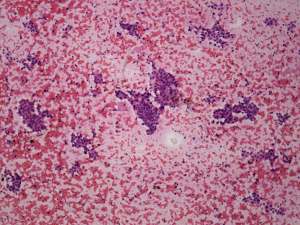
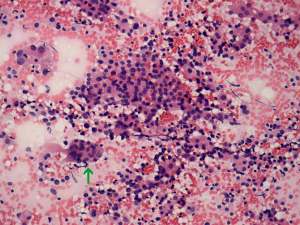
Cytology of the hypoechoic lesion disclosed Hashimoto's thyroiditis and Hürthle-cell proliferation from the lesion in the right lobe.
We advised regular follow-up examinations instead of a surgery. The patient asked whether we can exclude the possibility of malignancy with 100%. We had to answer the question: the risk of malignancy is not greater than 1%. The patient decided to undergo surgery.
Histopathology: benign, Hashimoto's thyroiditis. There were several areas partly divided by fibrous tissue but these corresponded neither hyperplastic nodule nor a Hürthle-cell tumor.
Comments.
-
Fortunately, patients rarely ask in a wrong way. In this case we had to answer a wrong question. Naturally, we cannot exclude the possibility of malignancy. Our explanation, that a regular follow-up instead of an immediate surgical procedure would be a safe method, was not enough to decrease the anxiety of the woman from having a malignant disease.
-
Most discrete lesions were clearly not true nodules. The hypoechoic one in the right lobe and the hyperechoic one in the lower pole of the left lobe could be pathological nodules on their ultrasound presentation. However, in neither case would I advise calling it a nodule in the ultrasound report. In this case, the use of a nodule-like or discrete lesion is appropriate.