
|
|
Study on 100 consecutive patients with thyroid nodule - case 032
|
|







Clinical presentation: A 51-year-old man requested a second opinion. He has been treated for malignant melanoma 18 months. On chest X-ray examination a substernal thyroid was discovered. Aspiration cytology from the right lobe resulted in benign lesion. The patient had no compression signs, although X ray examination disclosed a 50% narrowing of the trachea. He has got inconsistent information regarding the extent of surgery.
Palpation: a firm enlarged right thyroid was palpable.
Functional state: euthyroidism (TSH 2.59 mIU/L).
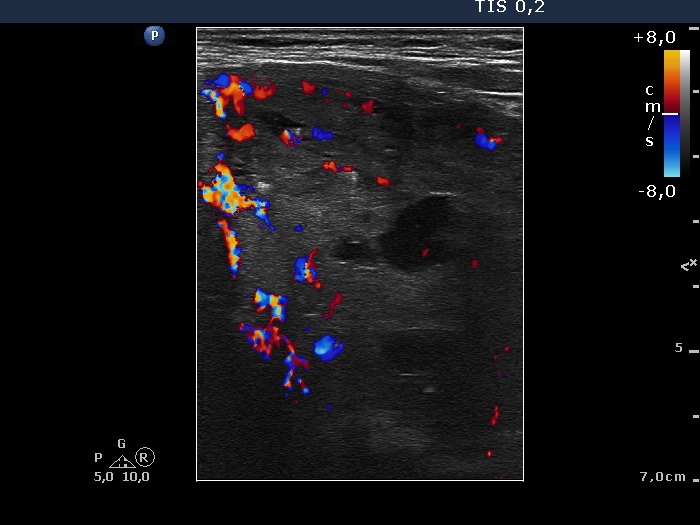
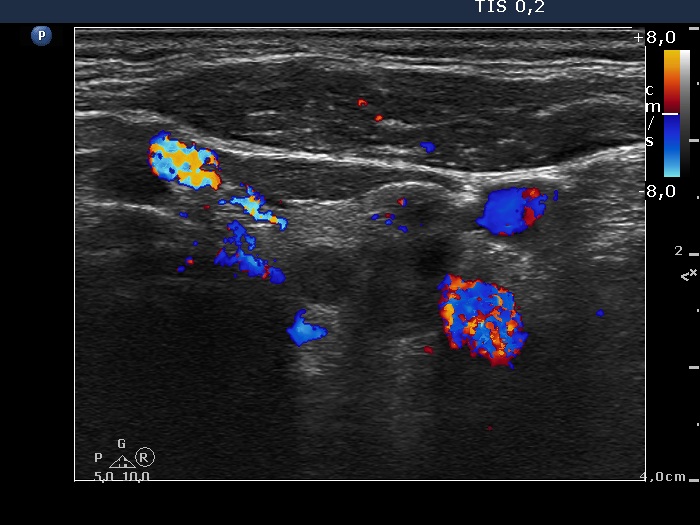
Ultrasonography. The right thyroid was composed of multiple discrete lesions with different echogenicities. The lobe was extremely enlarged with the dimension of 55x65 xminimum 120 mm (width, depth, and length, respectively) and spread retotracheal and substernal. The lower pole of the lobe could not be visualized while swallowing. The left thyroid was normal-sized and contained several hypoechogenic lesions. There was a moderately hypoechogenic nodule in the right lobe. The lesion presented neither halo nor perinodular blood flow.
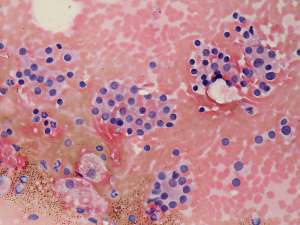
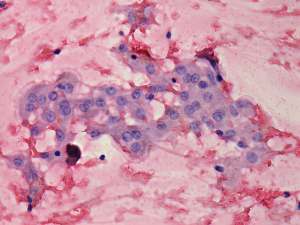
Cytology was performed from a hypoechogenic nodule in the left lobe and resulted in benign, colloid goiter.
We advised a right lobectomy. As regards the left lobe we explained the patient that he has to decide whether to remove this lobe or to leave intact. All in all, I advised to remove only the right thyroid.
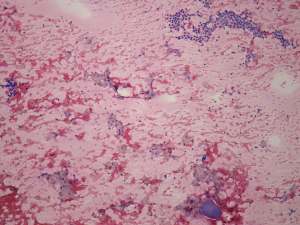
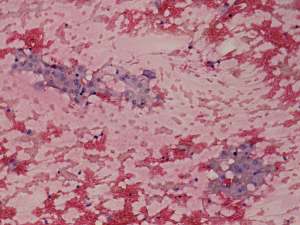
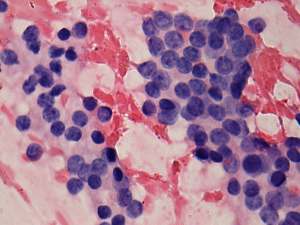
Right lobectomy was performed and histopathology disclosed benign hyperplastic nodules and a focus of a solitary papillary microcarcinoma with 2 mm in maximal diameter.
Comments.
- In our opinion, the patient has to decide whether to undergo on lobectomy or total thyroidectomy in those cases when there is an unequivocal need of an unilateral lobectomy and the other lobe contains smaller lesions which itself does not constitute an indication of surgery. We have to give all information to this decision. A total thyroidectomy ensures that the patient will not require a second operation during the whole lifetime. On the other hand, the risk of a bilateral recurrent nerve damage has to be considered, similarly to the mostly psychological drawback of a life-time replacement therapy. If only an unilateral lobectomy would be performed, than a repeat surgery might be required decades later if the nodules in the left lobe would be increase.
- In this case we favored the unilateral lobectomy because of the significantly increased risk of recurrent nerve damage during operation. Note that the right lobe was around 50-times enlarged in volume and spread substernal and retortracheal. Such extreme goiters significantly increase the risk of recurrent nerve damage.