Chronic lymphocytic thyroiditis - Case 29 |
Clinical presentation: neck dyscomfort and fever lasting for 3
weeks.
Laboratory data: mild hyperthyroidism with
TSH 0.05 mIU/L, FT4 30.1 pM/L, FT3 8.99 pM/L, aTPO 2 U/mL, TSAb
negative, erythrocyte sedimentation rate 31 mm/H, CRP 8,9 mg/l (normal
values: 0-4.8).
|
 |
 |
 |
 |
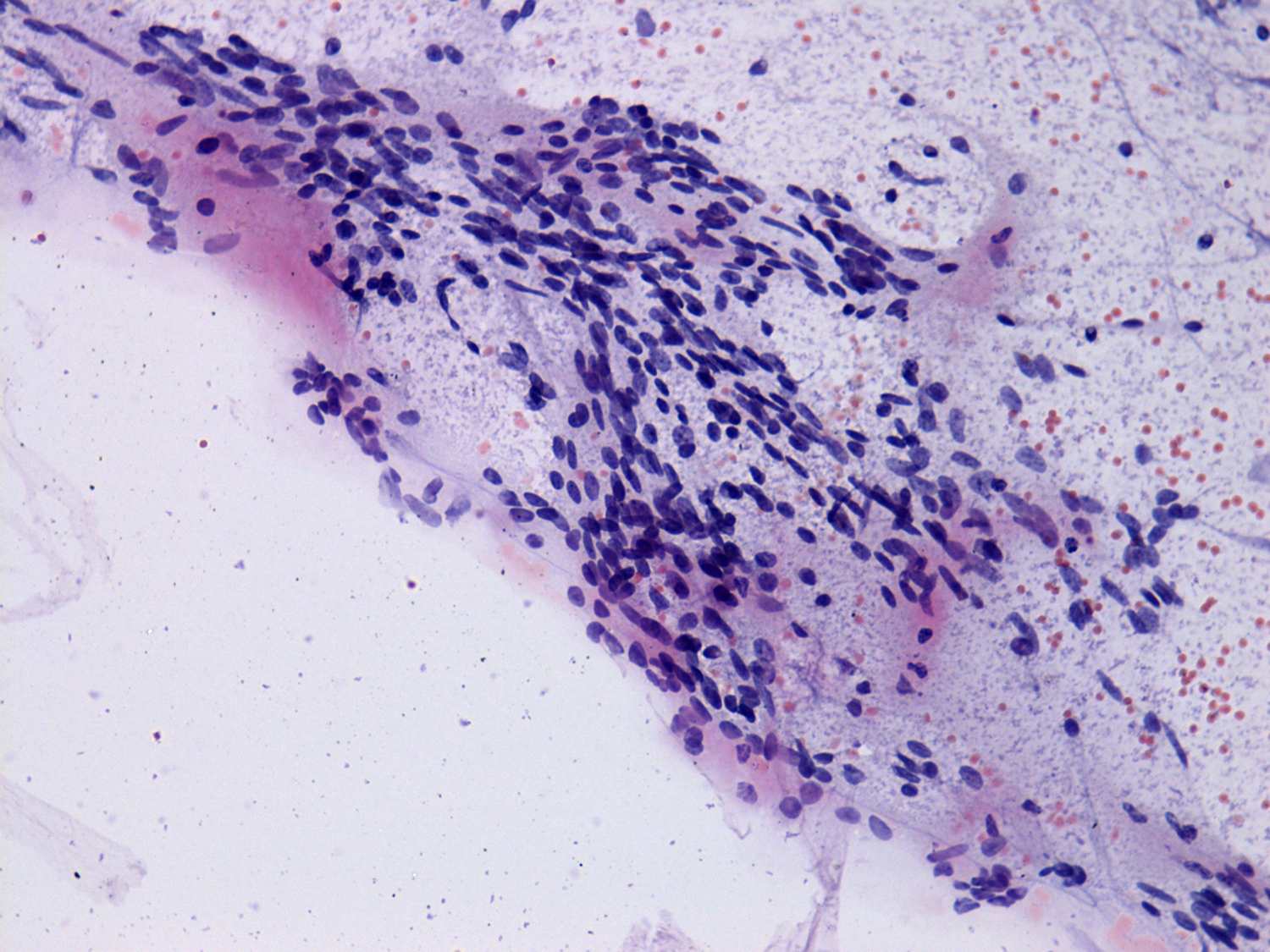
The cytological pattern is consistent with de Quervain's thyroiditis.
Two multinucleated giant cells are presented, both of them are composed
of epitheloid cells.
|
|
Right lobe
|
Left lobe
|
 |
 |
 |
 |
 |
 |
|
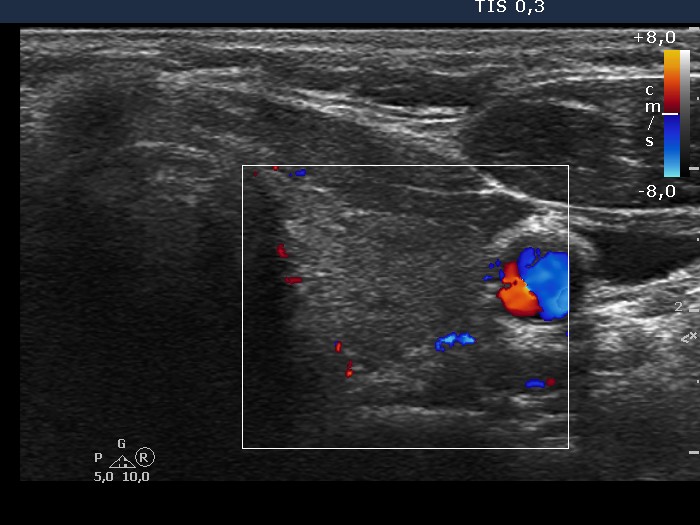
The sonographic presentation strongly argues against the possibility of
de Quervain's thyroiditis. First, there is no difference between the
two lobes. Second, the hypoechogenic areas have sharp, puzzle-like
borders, and third, the vascularization is increased.
|
|
Our final diagnosis was Hashimoto's thyroditis and hashitoxicosis. The
follow-up results, including the development of severe spontaneous
hypothyroidism and the elevation of aTPO level 6 months later, verified
this. Nevertheless, we cannot exclude the possibility that the patient
had initially a de Quervain's thyroiditis, too.
|
|
