Intranodular hyperechogenic figures - Table 10 (large). Differentiation of nodules presenting hyperechogenic granules |
||
Although the analysis of hyperechogenic granules is very important when we judge a nodule, there are other features takenwhich must be take into account during the interpretation of a nodule. We have to consider all of these characteristics in differential diagnostic methods. This analysis is of minimal importance until we have the opportunity and freedom to perform aspiration cytology even from the least suspicious nodule. However, the current trends try to minimize the ratio of unnecessary FNAs which put a greater responsibility on the shoulder of the ultrasonographer.
Hashimoto's thyroiditis (cytological diagnosis) - case 1137 |
Papillary carcinoma (histological diagnosis) - case 1627 |
 |
 |
|
 |
|
|
|
|
Oxyphilic adenoma - case 60 |
Papillary carcinoma - case conp 078 |
 |
 |
 |
 |
|
|
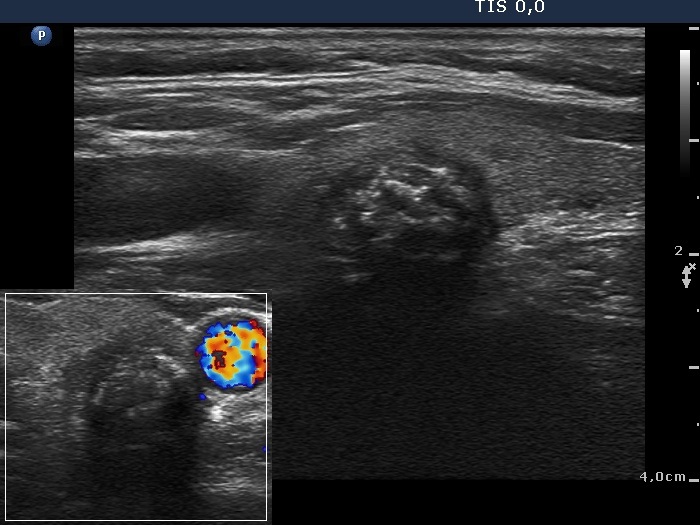
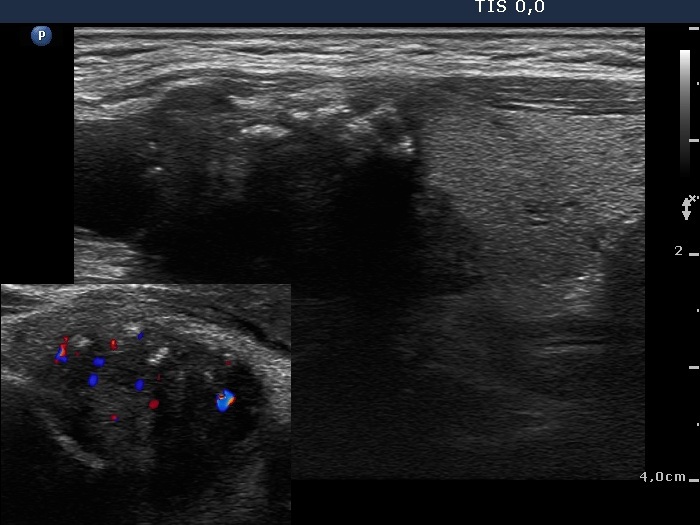
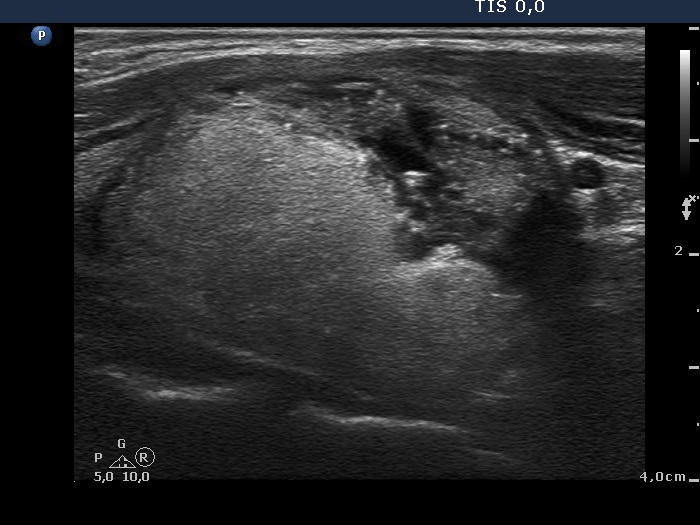
Intrathyroidal parathyroid adenoma (histological diagnosis) - case 1399 |
Papillary carcinoma (histological diagnosis) - case conp 031 |
 |
 |
|
 |
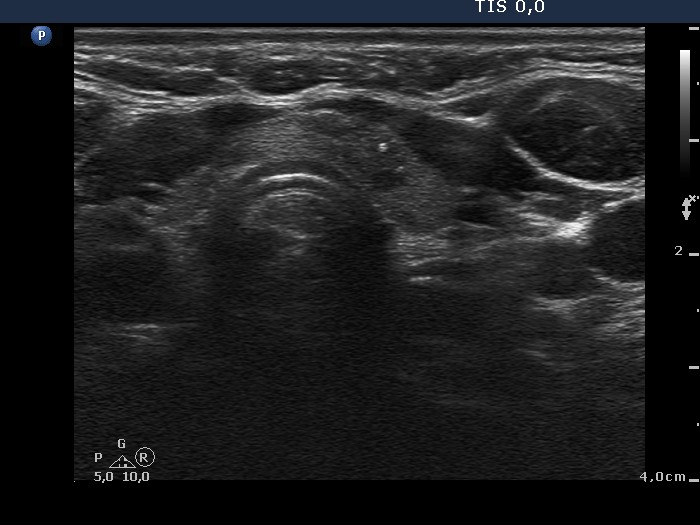
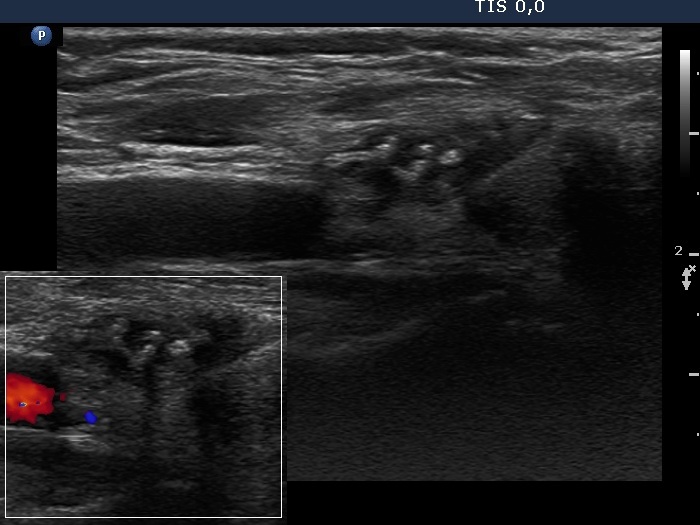
There are a few hyperechogenic granules within the small parathyroid lesion and we can see two much thinner lines, as well. These figures might be either punctate echogenic foci or non-specific granules. The papillary carcinoma contains punctate echogenic foci. The main differences between the appearance of the cases are the shape and borders: regular and sharp in the left benign, while irregular, blurred in the right malignant focus. |
|
Benign colloid goiter - case cons100_001 |
Papillary carcinoma (histological diagnosis) - case conp 035 |
 |
 |
 |
 |
|
|
Benign hyperplastic nodules (histological diagnosis) - case 444 |
Papillary carcinoma (histological diagnosis) - case conp 002 |
 |
 |
 |
 |
|
|
Oxyphilic adenoma (histological diagnosis) - case 1735 |
Papillary carcinoma (histological diagnosis) - case conp 050 |
 |
 |
 |
 |
|
|
Benign hyperplastic nodule (histological diagnosis) - case 80 |
Papillary carcinoma (histological diagnosis) - case conp 057 |
 |
 |
 |
 |
|
|
Benign hyperplastic nodule (histological diagnosis) - case 1091 |
Benign hyperplastic nodule (histological diagnosis) - case conp 026 |
 |
 |
 |
 |
|
|
Benign hyperplastic nodule (histological diagnosis) - case cons100_024 |
Papillary carcinoma (histological diagnosis) - case conp 005 |
 |
 |
 |
 |
|
|
Follicular adenoma (histological diagnosis) - case 11 |
Papillary carcinoma (histological diagnosis) - case conp 009 |
 |
 |
 |

|
|
|
Granulation around surgical thread (cytological diagnosis) - case 1343 |
Papillary carcinoma (histological diagnosis) - case conp 045 |
 |
 |
 |
 |
|
|
Granulation around surgical thread (histological diagnosis) - case 411 |
Papillary carcinoma (histological diagnosis) - case 779 |
 |
 |
 |
 |
|
|
Oxyphilic adenoma (histological diagnosis) - case 368 |
Papillary carcinoma (histological diagnosis) - case conp 028 |
 |
 |
 |
 |
|
|
Follicular adenoma (histological diagnosis) - cons_operated case 072 |
Follicular adenoma (histological diagnosis) - case 424 |
 |
 |
 |
 |
|
|
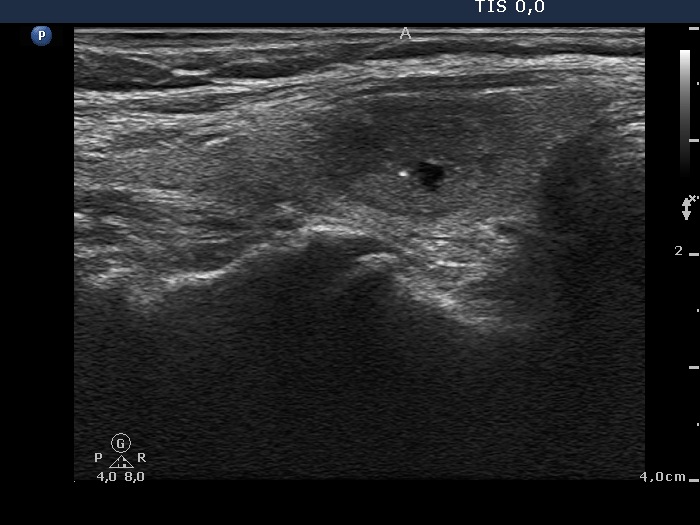
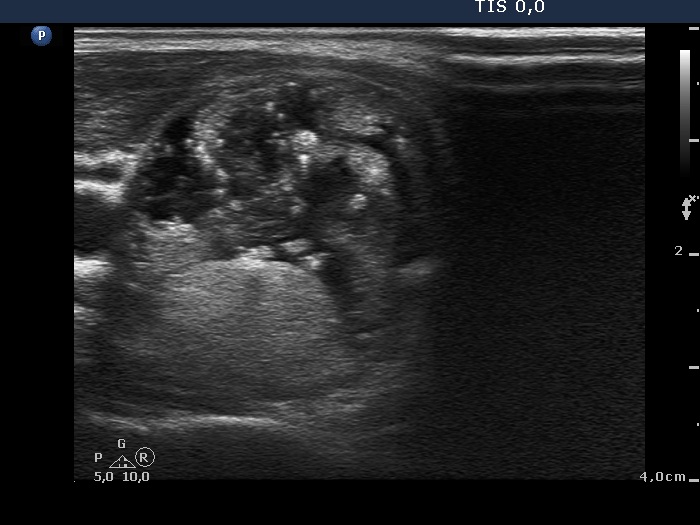
Benign colloid goiter (cytology) - case 1332 |
Papillary carcinoma (histological diagnosis) - case conp 027 |
 |
 |
 |
 |
The nodule presented in these cases are very similar, indeed there is no obvious difference between the presentations. The brightest echogenic spots are punctate echogenic foci in both cases. While the less bright lines and granules correspond to back wall figures. |
|