
|
|
The borders of the nodule - case 1484
|
|







Clinical presentation: A 55-year-old woman was referred for aspiration cytology. She was treated for hyperthyroidism caused by Graves' disease 2 years ago. Scintigraphy was performed at the beginning of hyperthyroidism and resulted in elevated uptake. No nodule was detected. Ultrasound was not performed. Recently, the patient felt neck discomfort and ultrasound disclosed a suspicious nodule.
Palpation: The presence of nodules was doubtful in both lobes.
Functional state: euthyroidism (TSH 0.93 mIU/L, FT4 14.1 pM/L).
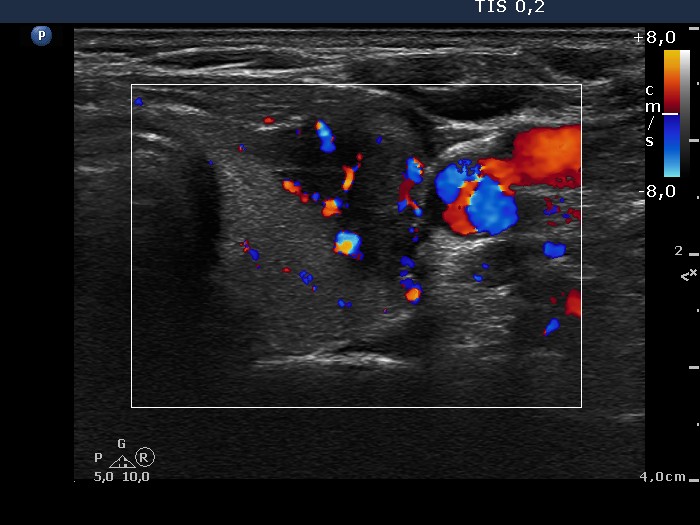
Ultrasonography: Both lobes were echonormal. The ventral surface of the right lobe was uneven which caused the nodular appearance on palpation. There was a hypoechogenic nodule in the left thyroid. The nodule had blurred and lobulated borders and displayed irregularly increased intranodular blood flow.
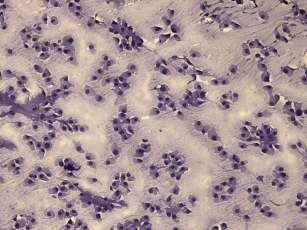
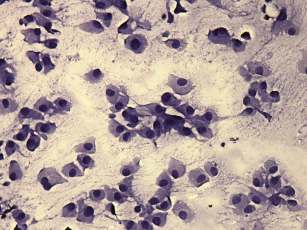
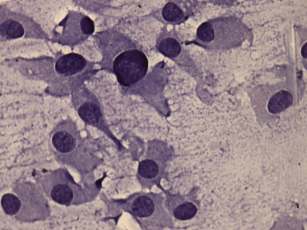
Cytological report: suspicion of malignancy. Medullary cancer or a Hürthle-cell tumor should be considered.
Serum calcitonin was measured and was in normal range.
Combined clinical-sonographic-cytological diagnosis: Hürthle-cell tumor with greater than the average risk for malignancy.
Histopathology disclosed Hürthle-cell adenoma.
Comments.
-
In a nodule with such an ultrasound presentation, i.e. a deeply hypoechogenic pattern, blurred and lobulated borders, subacute thyroiditis and papillary carcinoma have to be considered.
-
The cytological presentation is also suspicious. Polygonal, even triangular forms were found, which raised the possibility of medullary carcinoma. However, the nucleo-cytoplasmatic ratio is less than in medullary carcinoma.