
|
|
The role of complex diagnosis - follow-up of follicular lesions - Case 3.
|
|











First examination (1st and 2nd rows of images)
Clinical presentation: a 44-year-old man was referred for cytological evaluation of a thyroid nodule discovered on screening. Scintigraphy indicated a cold nodule. He has no complaints.
Palpation: a solitary firm nodule in the right lobe.
Hormonal examination: euthyroidism with TSH-level 0.38 mIU/L.
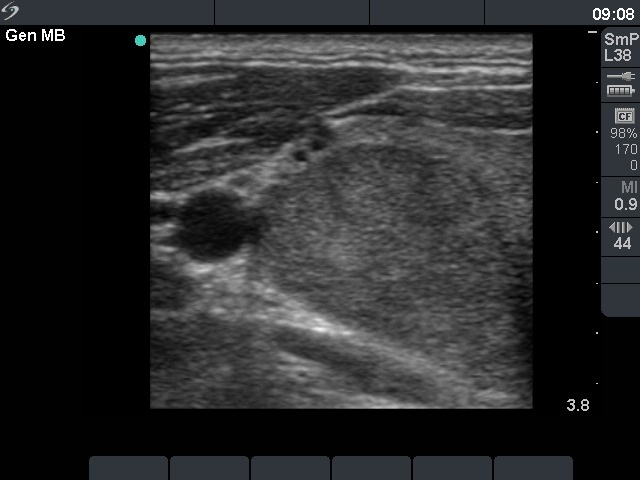
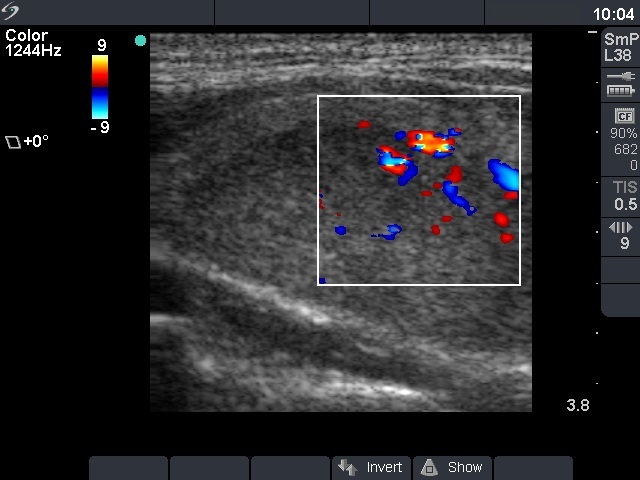
Ultrasonography. There was a solitary moderately hypoechogenic nodule in the right lobe with a halo sign and perinodular blood flow.
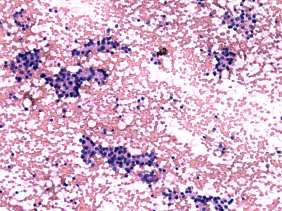
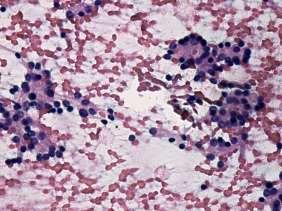
Cytological report follicular tumor.
I advised surgery but the patient had great fear from operation. He asked me how to avoid surgery. I told him that it is hard to explain that he can avoid surgery within a decade but considering the not greater than 2% risk of carcinoma, the postponement of the decision about operation shares minimal if any risk if he undergoes on yearly ultrasound examination.
Second examination 18 month later (3rd row of images)
Clinical presentation: the patient had no complaints.
Palpation: a solitary firm nodule in the right lobe.
Hormonal examination: euthyroidism with TSH-level 0.61 mIU/L.
Ultrasonography. There was a solitary moderately hypoechogenic nodule in the right lobe with a halo sign and perinodular blood flow. The nodule has increased in volume with 84% compared with first examination.
Considering the remarkable increase in nodule size I told the patient that further delay in surgical treatment shares significant risks.
A right lobectomy was performed. Histopathology disclosed follicular adenoma.