
|
|
The role of complex diagnosis - oxyphilic lesions - Case 1.
|
|






Clinical presentation: a 53-year-old woman was referred for a regular follow-up examination. She was operated on a benign nodular goiter for 19 years. She had no complaints.
Palpation: a nodule in the left lobe.
Functional state: euthyroidism with TSH-level 0.41 mIU/L, FT4 14.2 pM/L.
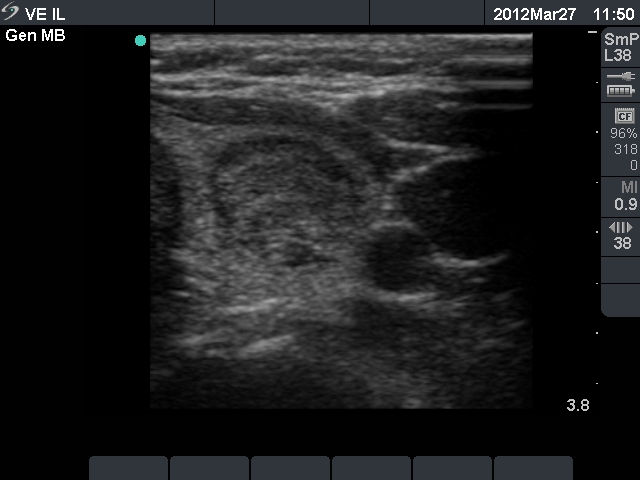
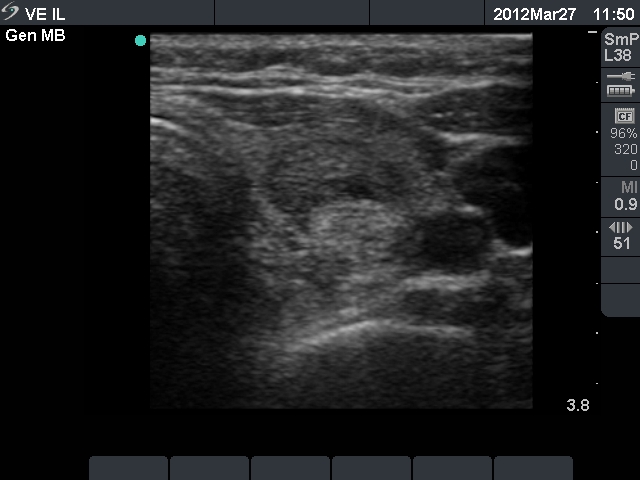
Ultrasonography: the thyroids were echonormal and contained multiple small hypoechogenic lesions. There was a mixed moderately hypoechogenic-echonormal nodule in the left lobe. The nodule exhibited a halo sign and peri- and intranodular blood flow.
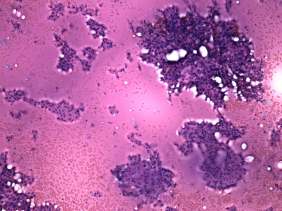
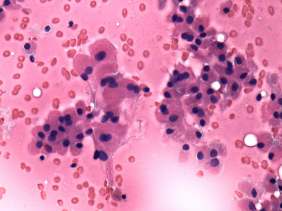
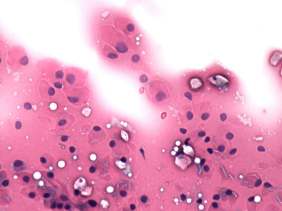
Cytological picture: there was diffuse colloid precipitate in the background. Beside compact clusters of follicular cells many isolated follicular cells were found. Thyrocytes partly exhibited oxyphilic metaplasia, but did not contain prominent nucleoli.
Cytological diagnosis: benign colloid goiter with oxyphilic metaplasia.
We offered regular follow-up examinations. Two years later the patient was examined in another hospital. The size of the nodule did not change. FNAC was performed and because of the presence of oxyphilic cells cytology resulted in suspicion of malignancy, and an "immediate surgery" was suggested.
The patient visited me again with great anxiety later. Although, I told her my unequivocal opinion that her nodule is benign, I had to offer surgery because of judiciary and psychological reasons.
Histopathology: benign hyperplastic nodule with focal lymphocytic thyroiditis.
Comment: this is an extremely rare situation that malignancy evolves in a patient who was previously operated for a benign multinodular goiter. It is also extremely unlikely that a mixed hypoechogenic (not cystic)-echonormal nodule would be malignant. The fact that the nodule did not increase in size over years, is also a very strong argument against malignancy. And last, the presence of colloid and the lack of prominent nucleoli also stand against malignancy. Taking these into account: giving a suspicious diagnosis under these circumstances is a mistake.
Nevertheless, the cytological picture itself may be disconcerting. But the cytopathologist, the clinician and the radiologist should be members of a team and except for ambiguous situations, they have to give a shared diagnosis considering all circumstances.
This case is enlisted among Benign nodular hyperplasia - Case 40, too.