
|
|
The role of complex diagnosis - oxyphilic lesions - Case 2.
|
|









First examination (1st and 2nd rows of images)
Clinical presentation: a 26-year-old woman was referred for evaluation of a hypothyroidism. She was investigated because of infertility.
Palpation: the isthmic part of the right lobe was firm.
Functional state: hypothyroidism on daily 25 microgram levo-tiroxine with TSH-level 14.5 mIU/L, FT4 8.79 pM/L, anti-TPO 618 U/mL.
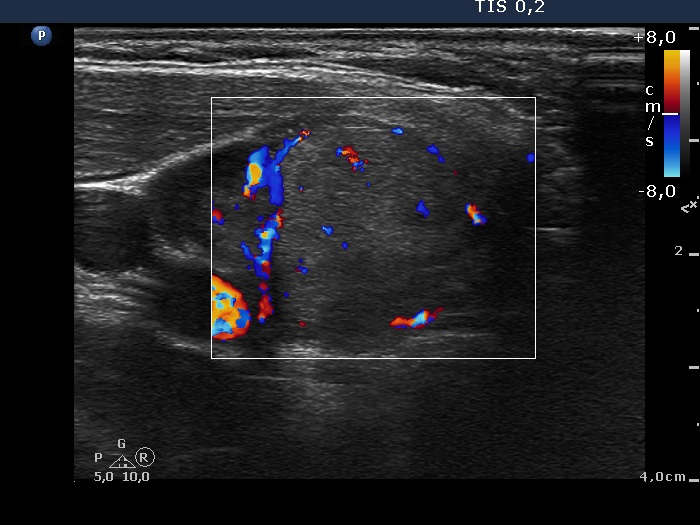
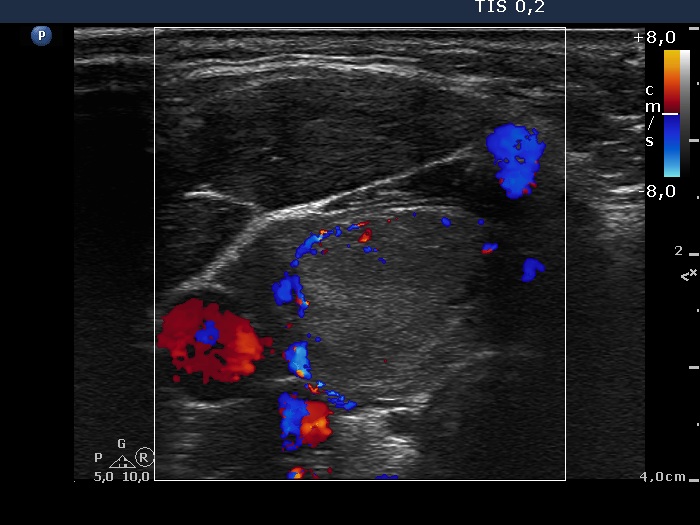
Ultrasonography : the thyroid was hypoechogenic. The right lobe presented two echonormal areas. The larger was suspicious being a nodule in pathological sense. The lesion displayed signs of a type 2 vascular pattern.
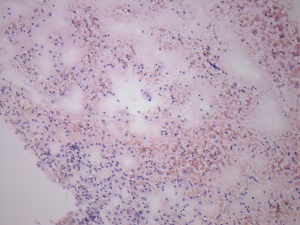
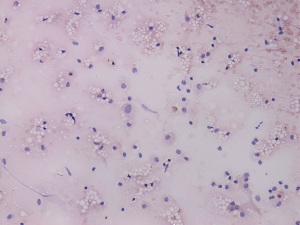
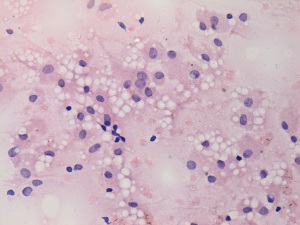
Cytology was performed and resulted in Hashimoto's thyroiditis and proliferation of oxyphilic cells.
A combined clinical-ultrasound-cytological diagnosis was hypothyroidism caused by autoimmune thyroiditis. Thyroid nodule in question with less than 1% risk of carcinoma.
Replacement therapy was started. As regards the lesion in question, we advised the patient follow-up instead of immediate surgery.
Follow-up examination 2 years later (3rd row of images)
Summary of follow-up: the patient underwent yearly ultrasound examination. The nodule was unchanged, she had no complaints. She visited us because she became pregnant.
Functional state: subclinical hypothyroidism on daily 100 microgram levo-tiroxine with TSH-level 5.08 mIU/L.
Ultrasonography: the ultrasound presentation of the thyroid was basically unchanged. Compared with the previous examination, the lesion in question presented more hypoechogenic areas and became less demarcated. The size of the lesion decreased significantly.
The volume of the nodule was 0.31 and 0.35 mL, at the first examination and at the 3-year follow up, respectively.Suggestion: to increase the levo-tiroxine dose to daily 125 microgram, checking the TSH 6 weeks later and continue the follow-up with ultrasound in two years.