
|
|
Chronic lymphocytic thyroiditis - Case 14.
|
|








Clinical presentation: a 51-year-old woman was referred for an evaluation of hypothyroidism detected on routine examination.
Palpation: the thyroids were firm, but no nodule was palpable.
Functional state: hypothyroidism with TSH 22.7 mIU/L, FT4 6.9 pM/L.
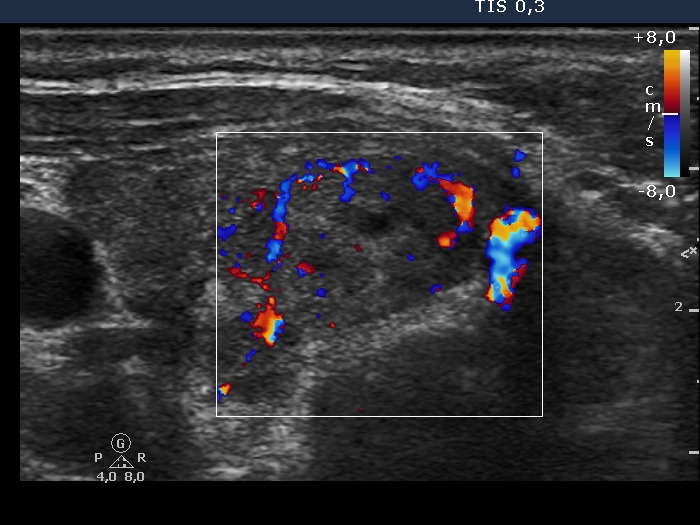
Ultrasonography: the thyroids were moderately hypoechogenic. There were numerous hyperechogenic areas. A larger, more hypoechogenic lesion was found in the lower pole of the right lobe. The lesion did not show a halo sign but had perinodular blood flow.
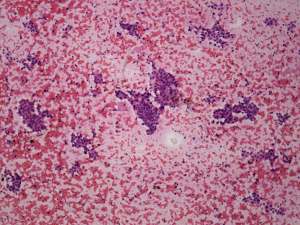
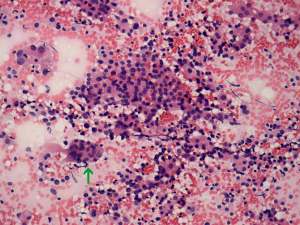
FNAC: disclosed Hashimoto's thyroiditis and Hürthle-cell proliferation from the lesion in the right lobe.
We advised regular follow-up examinations instead of a surgery. The patient asked whether we can exclude the possibility of malignancy with 100%. We had to answer the question: the risk of malignancy is not greater than 1%. The patient decided to undergo surgery.
Histopathology: benign, Hashimoto's thyroiditis. There were several areas partly divided by fibrous tissue but these fit neither hyperplastic nodule nor a Hürthle-cell tumor.
Comment: fortunately, patients rarely ask in a wrong way. In this case we had to answer a wrong question. Naturally, we cannot exclude the possibility of malignancy. Our explanation, that a regular follow-up instead of an immediate surgical procedure would be a safe method, was not enough to decrease the anxiety of the woman from having a malignant disease.