
|
|
The operated thyroid - Case 23.A patient after a lobectomy
|
|








First examination - before surgery (first and second rows of images)
Clinical data: a 36-year-old woman was referred for evaluation of a subclinical hyperthyroidism. She was investigated because of elevated blood pressure.
Palpation: there was a relatively large nodule in the right thyroid.
Result of blood tests: subclinical hyperthyroidism (TSH 0.01 mIU/L, FT4 16.2 pM/l, FT3 5.93 pM/L).
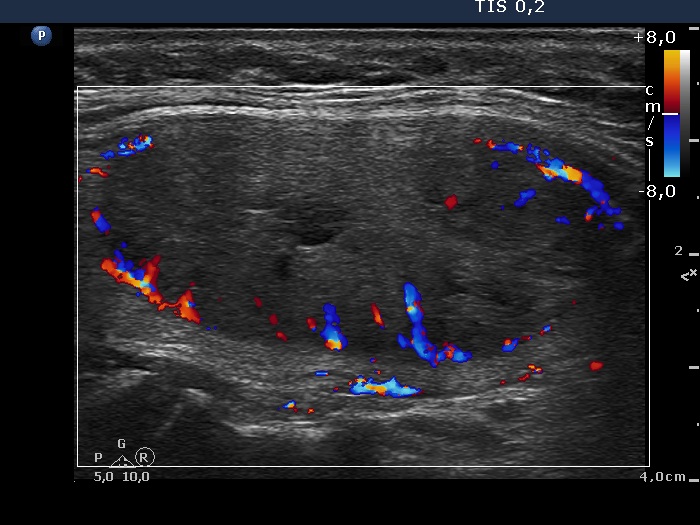
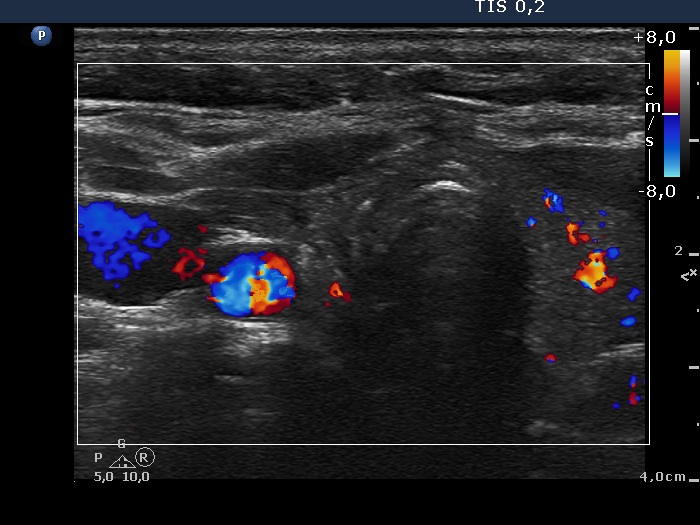
Ultrasonography: there was moderately hypoechogenic, inhomogeneous nodule presenting type 2 vascular pattern but not a halo sign in the right lobe. The left thyroid was atrophic with a small hypoechogenic lesion.Taking the previous data into account, the likelihood of an autonomously functioning adenoma was more than 95%. We sent the patient for radioiodine therapy. Our presumed diagnosis was confirmed by pre-therapy iodine uptake determination. However, the dose requiring to a complete cure was relatively high and the patient decided to go on surgery.
Right lobectomy was performed. Histopathology disclosed follicular adenoma.
One year after surgery (third row of images)
Clinical data: the patient had no complaints.
Palpation: no abnormality.
Result of blood tests: euthyroidism (TSH 2.17 mIU/L).
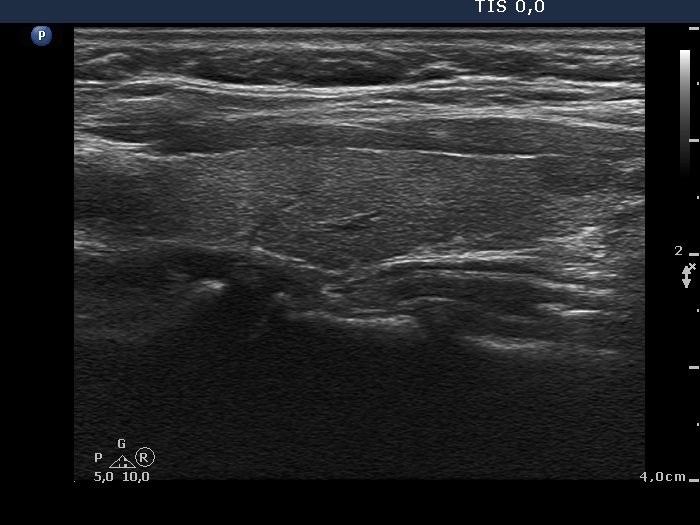
Ultrasonography. There was no parenchyma in the right thyroid bed. The left thyroid increased in size and became moderately hypoechogenic.Suggestion: yearly TSH determination, in the event of pregnancy at once. Ultrasound in every 3 to 5 years.
Comments.
-
The combination of a solitary nodule greater than 2 cm in maximal diameter with the atrophy of the contralateral lobe is highly suspicious for an autonomously functioning adenoma if the TSH is suppressed. The atrophy is caused by the low TSH level.
-
The echogenicity of the uninfluenced lobe frequently decreases after surgery. This may be caused by the changes in vascular supply.