
|
|
The role of complex diagnosis - oxyphilic lesions - Case 6.
|
|








First examination (1st and 2nd rows of images)
Clinical presentation: a 61-year-old woman was referred for evaluation of a hypothyroidism known for more than 15 years. She was treated with daily 75 microgram levo tiroxine and suffered from diffuse complaints.
Palpation: no abnormality.
Functional state: euthyroidism on daily 75 microgram levo-tiroxine with TSH-level 0.48 mIU/L.
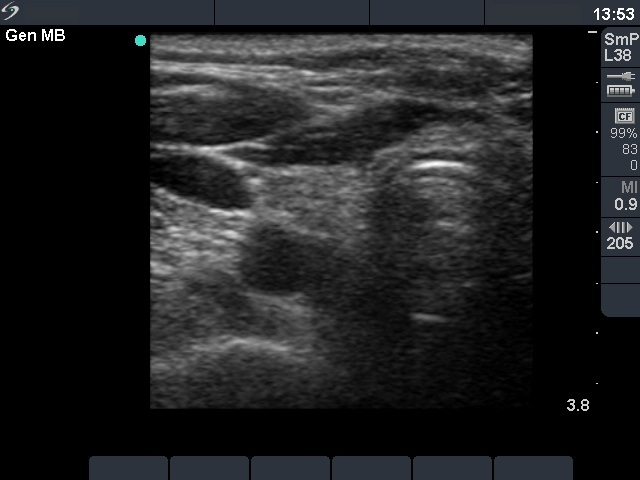
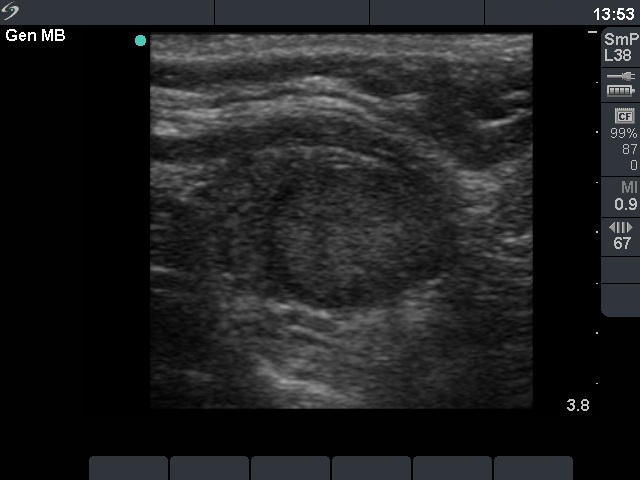
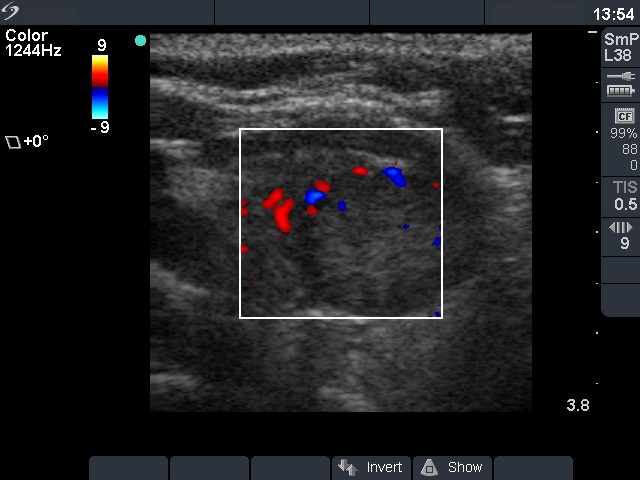
Ultrasonography: the right thyroid was atrophic. The left thyroid was composed of a central hypoechogenic nodule-like area surrounded with inhomogeneous parenchyma. The central lesion presented a type 2 vascular pattern.
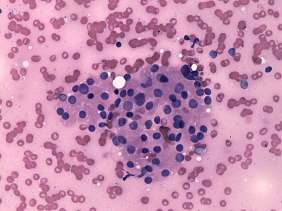
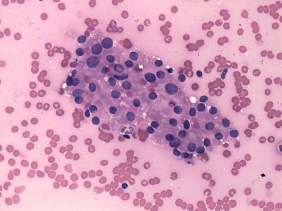
Cytology was performed from the lesion in the left lobe. The pattern corresponded to an oxyphilic cell lesions.
A combined clinical-ultrasound-cytological diagnosis was hypothyroidism caused by Hashimoto's thyroiditis and oxyphilic lesion with not greater than 1% risk of carcinoma.
We told the patient that the risk of carcinoma is very low and suggested yearly follow-up examinations.
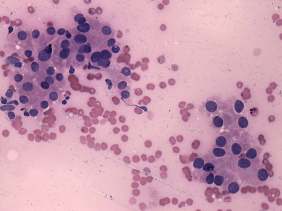
Follow-up examination 4 years later (3rd row of images)
Summary of follow-up: the patient underwent regularly ultrasound and TSH examination. The lesion in the left thyroid was unchanged. The patient suffered from diffuse complaints including fatigue, hair loss, weight gain, palpitation and 'lump in the throat' feeling.
Functional state: euthyroidism on weekly 750 microgram levo-tiroxine with TSH-level 0.38 mIU/L.
Ultrasonography: the basic ultrasound pattern of the thyroid was unchanged. The lesion in the right lobe increased with 46% which proved to be significant.
Cytology was repeated and resulted again in oxyphilic cell proliferation.
We suggested to continue follow-up. The patient asked whether an operation would resolve her complaints. We excluded this possibility. Nevertheless, the patient requested a second opinion and another endocrinologist advised surgery.
Histopathology disclosed Hashimoto's thyroiditis without any nodule in a pathological sense.
Comments.
-
A Hashimoto's thyroiditis may present in the form of a central large hypoechogenic area surrounded with a less hypoechogenic rim. This pattern is practically identical to a that of a large hypoechogenic nodule occupying great part of a lobe. It is doubtful on ultrasound whether this lesion is a nodule in a pathological sense or isn't.
-
The cytological pattern might correspond either to a Hürthle-cell tumor or to a Hashimoto's thyroiditis with oxyphilic cell proliferation.