
|
|
The role of complex diagnosis - oxyphilic lesions - Case 5.
|
|









First examination (1st and 2nd rows of images)
Clinical presentation: a 29-year-old woman was referred for evaluation of a thyroid nodule discovered by the patient herself. She was treated for hypothyroidism for 3 years.
Palpation: both thyroids were firm. An elastic nodule was palpable in the left thyroid.
Functional state: hypothyroidism on daily 50 microgram levo-tiroxine with TSH-level 11.7 mIU/L.
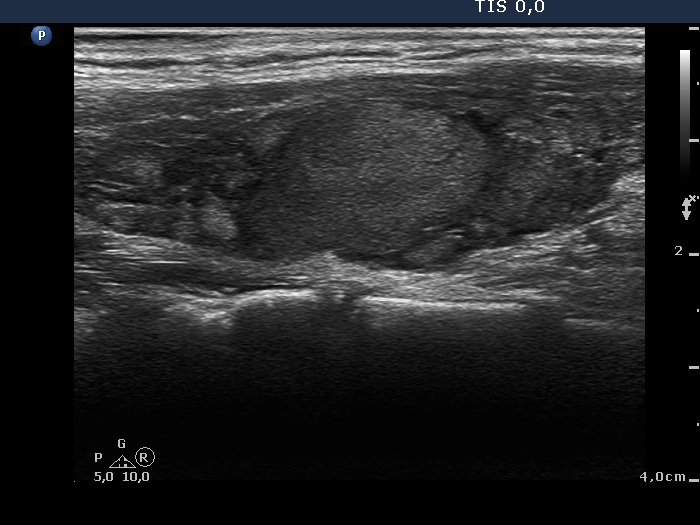
Ultrasonography: the thyroid was hypoechogenic and presented fibrosis. There was an echonormal lesion in the central part of the right thyroid while a mixed, spongiform cyst occupied great proportion of the left lobe. The lesion in the right lobe displayed a halo and perilesional blood flow.
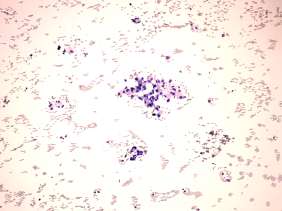
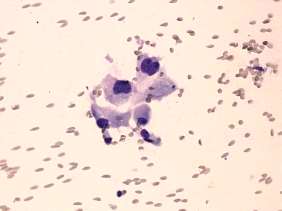
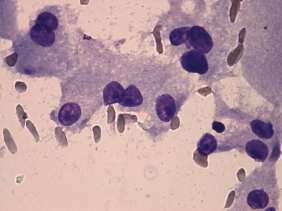
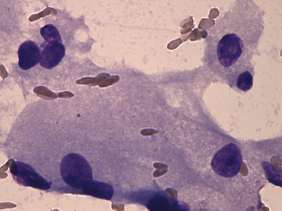
Cytology was performed from both lesions. The cytological pattern of the lesion in the right lobe is presented. It corresponded to an oxyphilic cell lesions. 6 mL cystic fluid was aspirated from the cystic nodule which disappeared after aspiration,
A combined clinical-ultrasound-cytological diagnosis was Hashimoto's thyroiditis and oxyphilic lesion with not greater than 1% risk of carcinoma.
We told the patient that the risk of carcinoma is very low and instead of immediate surgery, the decision can be postponed with regular follow-up. The patient decided to undergo regular follow-up (lesion in the right lobe) and sclerotherapy (nodule in the left lobe).
The cyst in the left thyroid has recurred 2 months later and this nodule was treated with percutaneous ethanol sclerotherapy. See case history in section Ethanol sclerotherapies..
Follow-up examination two years later (3rd row of images)
Summary of follow-up: the patient underwent regularly ultrasound and TSH examination. The nodule in the right lobe decreased gradually.
Functional state: euthyroidism on daily 100 microgram levo-tiroxine with TSH-level 0.96 mIU/L.
Ultrasonography: the basic ultrasound pattern of the thyroid was unchanged. Both the right thyroid and the lesion in the right lobe significantly decreased in size, the latter from 2.59 mL to 1.11 mL.
Suggestion: to continue the follow-up with ultrasound and TSH determinations every year.
Comments.
-
The cytological pattern itself corresponded to a Hürthle-cell tumor while the ultrasound presentation was equivocal. First, the lesion was echonormal. Second, similar echonormal lesions were found elsewhere in the thyroid. These echonormal areas might correspond to accentuated lobules less influenced by the underlying thyroiditis. Taking the results of follow-up into account, the lesion in the right lobe is probably not a nodule in a pathological sense while the risk of carcinoma can be excluded.
-
The decrease in size of the lobe and the lesion was the consequence of the normalization of the TSH. Similarly to other investigators, we tried to treat nodules with TSH suppressive therapy for 20 years. We found this therapy ineffective, the change in nodule size was similar to untreated nodule and we never ever met a nodule which decreased less than a half of the original on suppressive therapy.