
|
|
The role of complex diagnosis - follicular proliferation - Case 6.
|
|









Clinical presentation: a 56-year-old woman was referred for an evaluation of a nodule discovered by screening.
Palpation: a not firm nodule in the left lobe.
Hormonal examination: indicated euthyroidism with TSH 2.19 mIU/L.
Ultrasonography. The thyroid was echonormal and contained hypoechogenic areas. The echogenicity index was 20%. There was an echonormal nodule in the left lobe. The lesions displayed halo sign and perinodular blood flow.
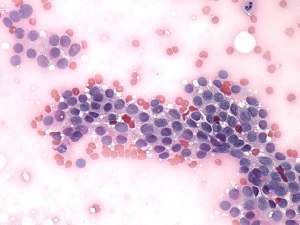
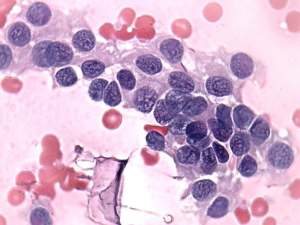
Cytology was performed and corresponded to a follicular tumor.
A combined clinical-ultrasound-cytological diagnosis was Hashimoto's thyroiditis and follicular proliferation with less than 1% risk of carcinoma.
Follow-up was advised with yearly ultrasound and TSH determination.
Comment.
-
The cytology is remarkable. Degenerative changes may cause irregular chromatin figures resembling groove. A typical groove is straight and starts at one side of the nucleus.
-
The risk of malignancy is very low in the event of an echonormal nodule. Combining the results of cytology and ultrasound, the risk of a follicular carcinoma is negligible in this patient.