
|
|
The role of complex diagnosis - follow-up of follicular lesions - Case 12.
|
|











First examination (1st and 2nd rows of images)
Clinical data: a 42-year-old man was referred for an evaluation of a thyroid nodule discovered by the patient himself.
Palpation: the right lobe was enlarged and contained a moderately firm nodule.
Functional state: euthyroidism with TSH 0.56 mIU/L
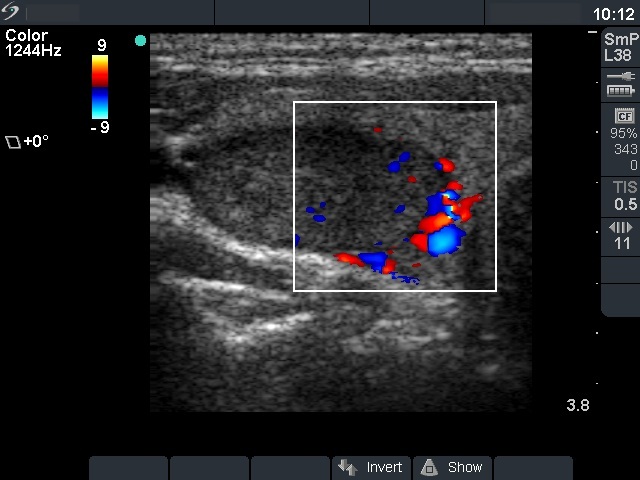
Ultrasonography: the thyroid was echonormal. A hypoechogenic nodule occupied great part of this lobe. The nodule presented a type 2 vascular pattern and displayed signs of intranodular vascularization. The nodule contained two more hypoechogenic areas which contained microcalcifications.
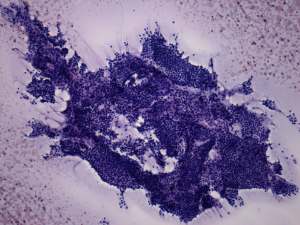
Cytological pattern corresponded to follicular proliferation without any significant atypia.
Combined clinical-ultrasound-cytological diagnosis: follicular tumor with not greater than 1% risk of malignancy.
We told the patient that he has the opportunity to choose between surgery and yearly follow-up investigation but considering the size of the lesion it seemed very likely that he has to be operated on later. He wished to avoid surgery.
Second examination 3 years later (3rd row of images)
Summary of follow-up: the patient underwent yearly ultrasound examination. At first examination the nodule increased in volume with more than 50% and surgery was initiated. Because of personal reasons the patient could not have surgery done so far.
Functional state: euthyroidism with TSH-level 0.70 mIU/L.
Ultrasonography: the ultrasound presentation of the thyroid was unchanged except for an increase in nodule volume to more than twice as the initial .
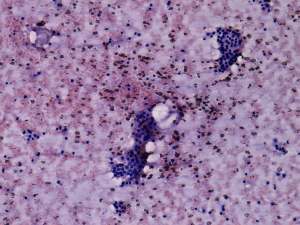
Cytology was repeated from the more hypoechogenic part of the nodule which presented microcalcifications and resulted in benign follicular proliferation.
A right lobectomy was performed and histopathology disclosed follicular adenoma.
Comment. The cytological pattern itself stands for a non-tumorous lesion: the presence of hyperplastic papillary fragments, that of naked pycnotic nuclei and colloid are specific features of a hyperplastic nodule. Microfollicular proliferation can be observed in practically each type of thyroid diseases. On the other hand, the ultrasound pattern is very suspicious for a follicular type tumor: a solitary large nodule presenting halo sign and perinodular blood flow is in more than 90% a follicular tumor.