
|
|
The role of complex diagnosis - follow-up of follicular lesions - Case 11.
|
|












First examination (1st and 2nd rows of images)
Clinical data: a 62-year-old woman was referred for an evaluation of a thyroid nodule known for more than ten years. Cystic fluid was aspirated two time from a nodule in the left lobe. She had no complaints.
Palpation: a moderately firm nodule in the left lobe.
Functional state: euthyroidism with TSH 1.83 mIU/L
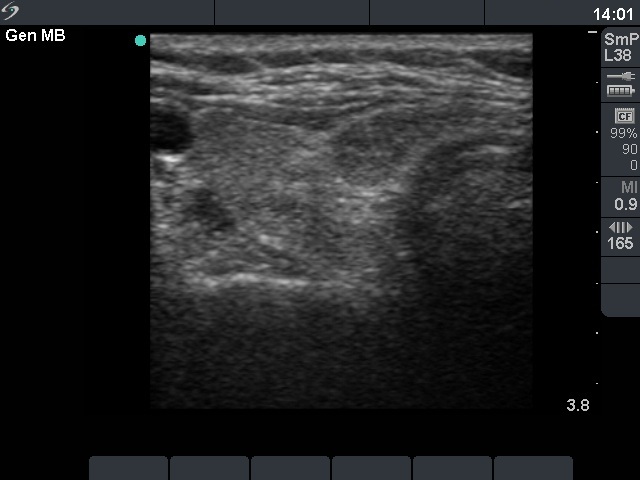
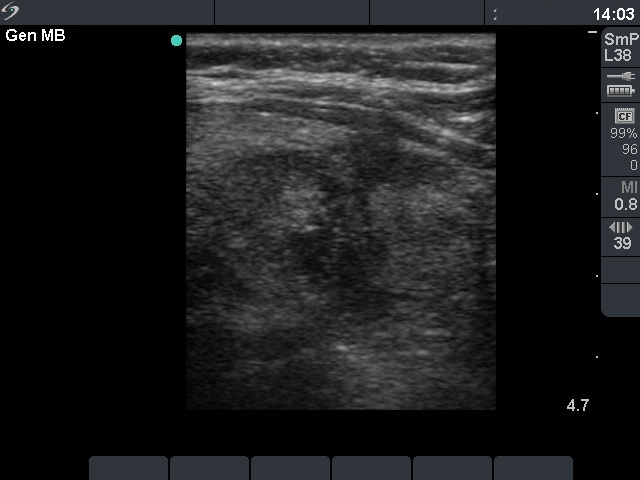
Ultrasonography: the thyroid was echonormal. There were several moderately hypoechogenic lesions in the right lobe, while the left lobe contained a larger nodular area composed of hyperechogenic and moderately hypoechogenic areas. The presence of a perinodular blood flow was doubtful.
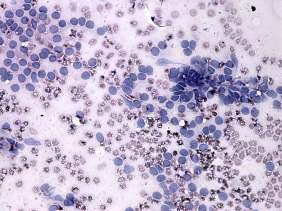
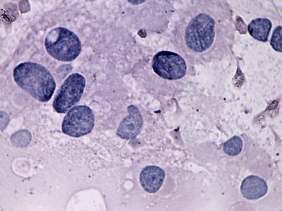
Cytology was performed form one of the moderately hypoechogenic areas in the right lobe and from the nodule in the left thyroid. The former resulted in benign colloid goiter while the latter in microfollicular proliferation without any significant atypia.
Combined clinical-ultrasound-cytological diagnosis: benign lesions in the right thyroid. A nodule in the left lobe with benign follicular proliferation.
Follow-up examination was suggested.
Second examination 3 years later (3rd row of images)
Summary of follow-up: the patient underwent yearly ultrasound examination. In the last six months she occasionally difficulties in swallowing and pressure symptoms in recumbent position.
Functional state: euthyroidism with TSH-level 0.70 mIU/L.
Ultrasonography: the ultrasound presentation of the thyroid was unchanged except for an increase in nodule volume to more than twice as the initial.
Cytology was repeated and resulted again in benign follicular proliferation.
Although tracheal X ray examination disclosed no obstruction we could not exclude the possibility that the compression sign were caused by the enlarging goiter.
Left lobectomy was performed and histopathology disclosed benign hyperplastic nodules.
3 months after surgery the patient was free of neck complaints.