
|
|
The role of complex diagnosis - follow-up of follicular lesions - Case 10.
|
|



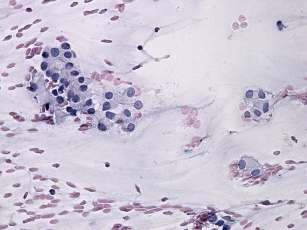

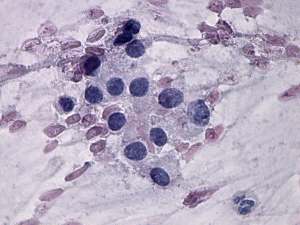




First examination (1st and 2nd rows of images)
Clinical presentation: a 37-year-old woman was referred for evaluation of nodular goiter known for 6 years. Scintigraphy disclosed a "cold" nodule and surgery was advised. The patient refused cytological examination. She had no complaints.
Palpation: a firm nodule in the right lobe.
Functional state: euthyroidism with TSH-level 0.71 mIU/L.
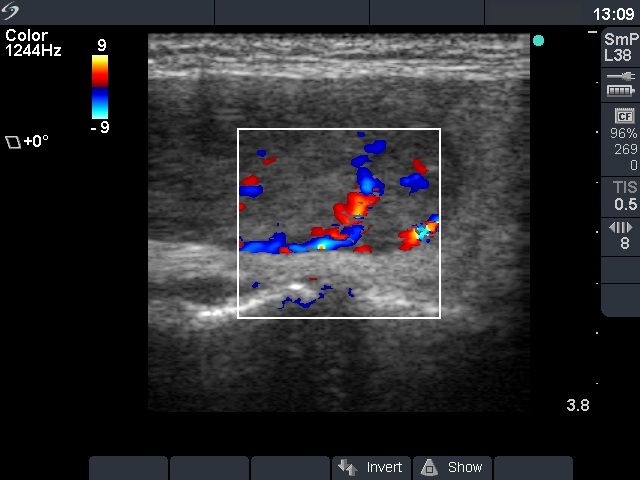
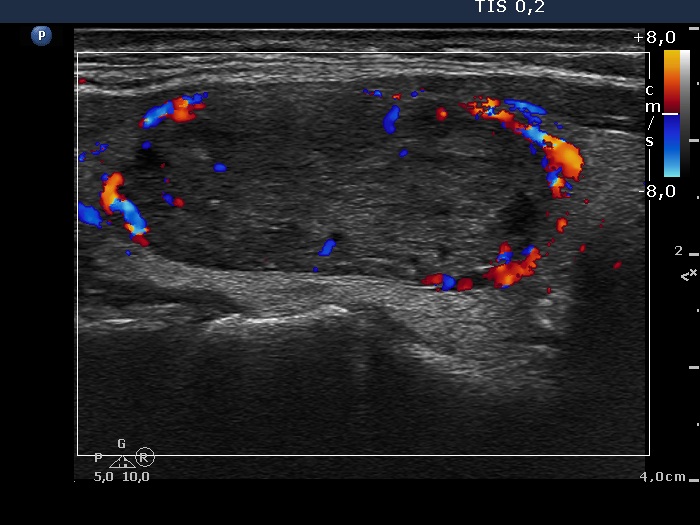
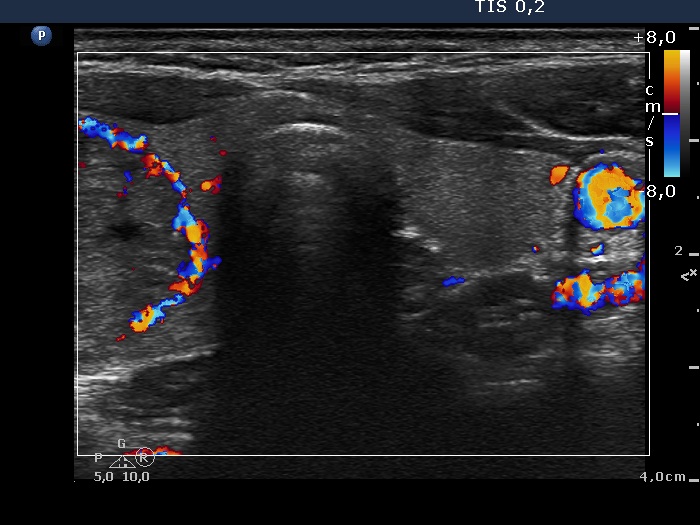
Ultrasonography. The thyroid was echonormal. There was a moderately hypoechogenic, inhomogeneous nodule in the right lobe. The lesion did not present a halo but did a perinodular blood flow.
Cytology was performed and pattern corresponded to a follicular tumor without significant atypia.
A combined clinical-ultrasound-cytological diagnosis was follicular tumor with less than 1% risk of carcinoma.
We advised surgery but told the patient that if she checks the nodule every year than the decision about surgery can be postponed until the nodule would not increase further.
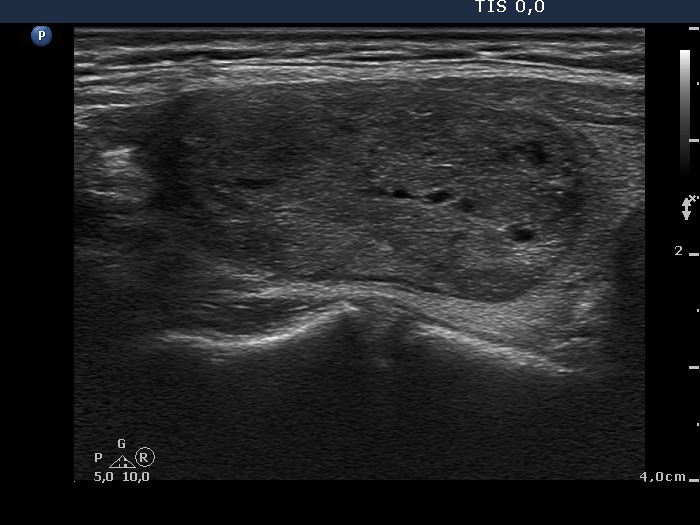
Follow-up examination 5 years later (3rd row of images)
Summary of follow-up: the patient underwent yearly ultrasound examination. The nodule was unchanged, she had no complaints.
Functional state: euthyroidism with TSH-level 0.93 mIU/L.
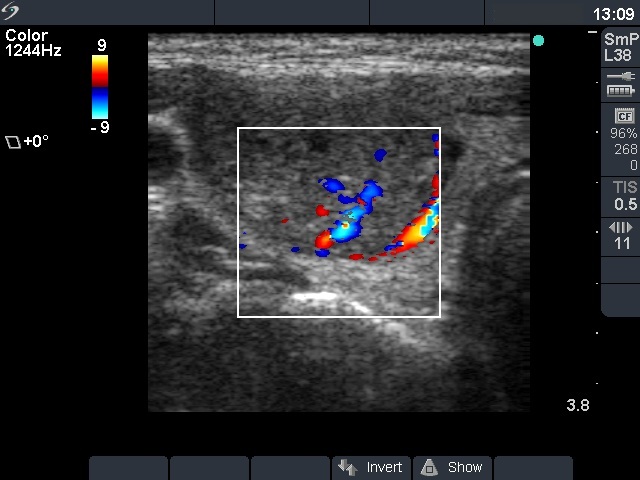
Ultrasonography: the ultrasound presentation of the thyroid was unchanged.
The volume of the nodule was 8.65 and 9.29 mL, at the first examination and at the 4-year follow up, respectively. The 7% increase in volume does not means a significant change.Suggestion: to continue the follow-up with ultrasound and TSH determinations every year.
Follow-up examination another 2 years later (3rd row of images)
Clinical presentation: the patient noticed pressure in supine position for several month.
Functional state: euthyroidism with TSH-level 0.82 mIU/L.
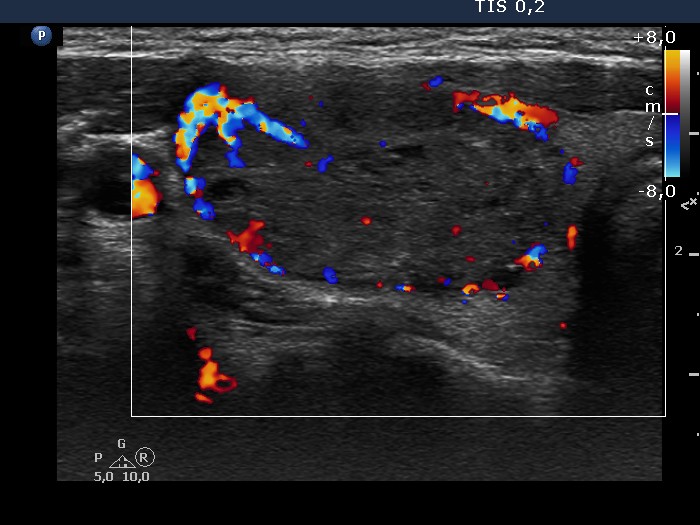
Ultrasonography: the ultrasound presentation of the thyroid was unchanged except for a significant increase in nodule size. The nodule increased by more than 60% compared to the previous examination.
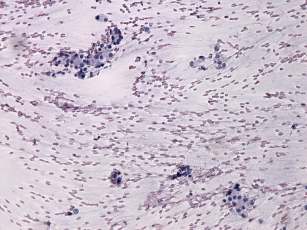
Cytology resulted in follicular tumor without atypia.
Suggestion: right lobectomy.
Histopathology disclosed follicular adenoma
Comment. The lack of halo in the presence of perinodular blood flow is a frequent finding in hypoechogenic nodules. The demonstration of a halo sign is very difficult or even impossible in most hypoechogenic nodules because the US appearance of the capsule in such lesions is identical with the nodule.