
|
|
Chronic lymphocytic thyroiditis - Case 31.
|
|









First examination (1st and 2nd rows of images):
Clinical presentation: a 39-year-old woman initiated a screening beacuse her mother was operated for a benign multinodular goiter. She had no complaints.
Palpation: no abnormality.
Functional state: hypothyroidism (TSH 35.2 mIU/L).
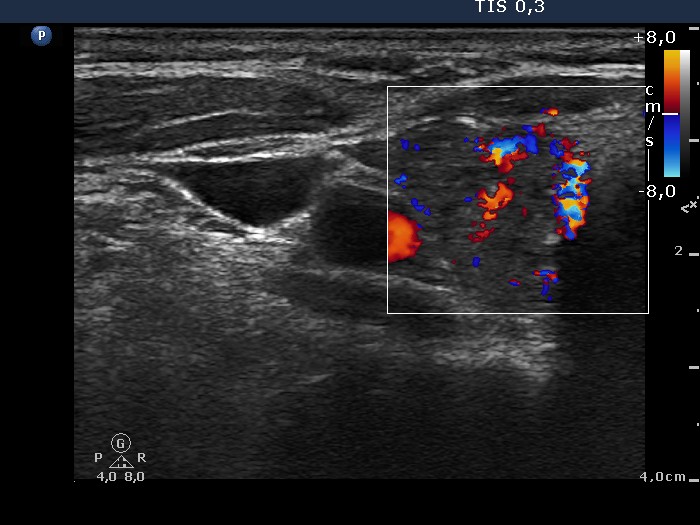
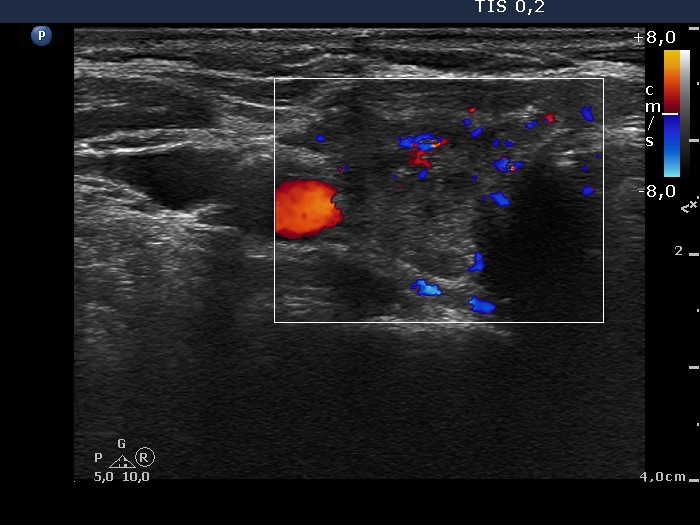
Ultrasonography: the basic echostructure of the thyroid was echonormal. There was a hypoechogenic lesion in the upper-ventral part of the right lobe. The lesion presented irregular, puzzle-like borders and hyperechogenic granules. There were moderately hypoechogenic circumscribed areas in the left lobe.
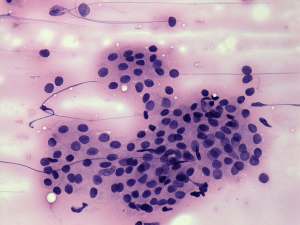
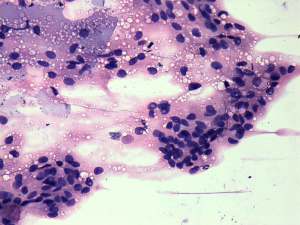
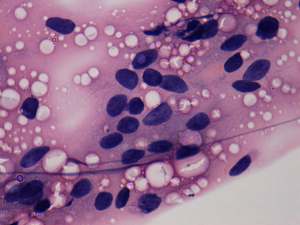
Cytology: performed from a hypoechogenic area in the right lobe and resulted in a benign colloid goiter and (focal) lymphocytic thyroiditis.
Anti-TPO: determined with an elevated result (398 U/mL).
Daily 100 microgram levo-tiroxin was administered in a gradually increasing dose.
Follow-up examination 18 months later (3rd row of images):
Clinical presentation: the patient felt much better. She told us that she did not notice prevously that her physical power and understanding was deteriorated.
Palpation: both thyroids were moderately firm.
Functional state: euthyroidism on daily 137.5 microgram levo-tiroxin (TSH 3.63 mIU/L).
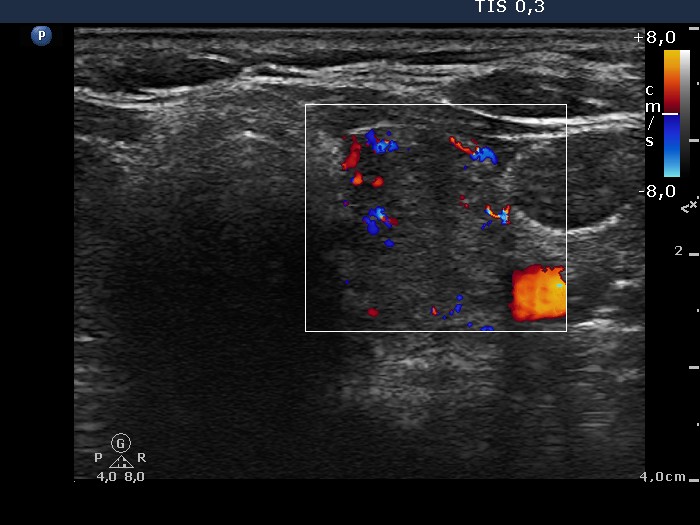
Ultrasonography. No significant change can be found. The thyroid became smaller but the difference in size is minimal. The echo pattern and the vascularization is the same..
Comments.
-
FNAC was performed because of psychological reasons: although the patient had no nodule, the previous sonographic report caused anxiety.
-
We can rarely find thick colloid in Hashimoto's thyroiditis.
-
In contrast with Graves' disease and de Quervain's thyroiditis, the sonographic pattern in Hashimoto's thyroiditis is stable and changes very slowly not over months or years but even over decades. The only exception is post partum thyroiditis.