
|
|
Graves' disease - Case 8.
|
|













First examination (first two rows):
Clinical presentation: a 51-year-old woman was referred for an evaluation of typical complaints suggesting hyperthyroidism.
Palpation: no abnormality.
Functional state: hyperthyroidism with TSH 0.001 mIU/L, FT4 71.4 pM/L.
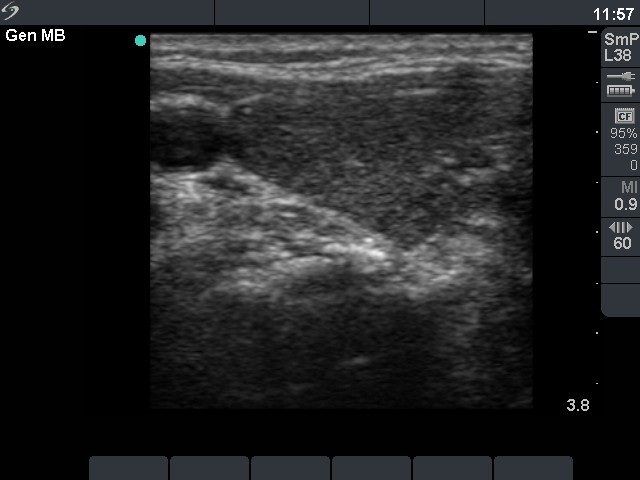
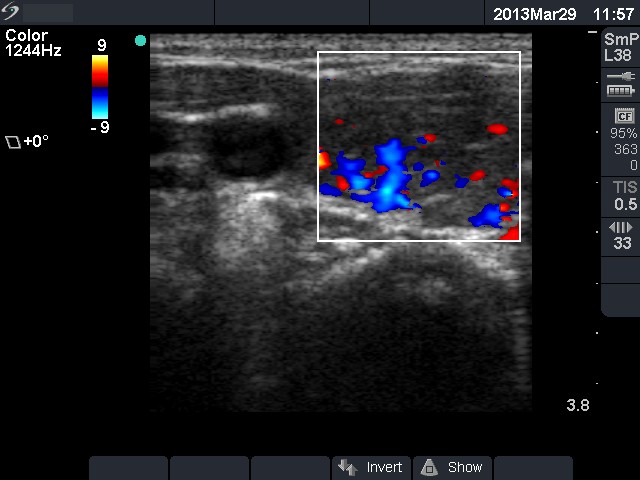
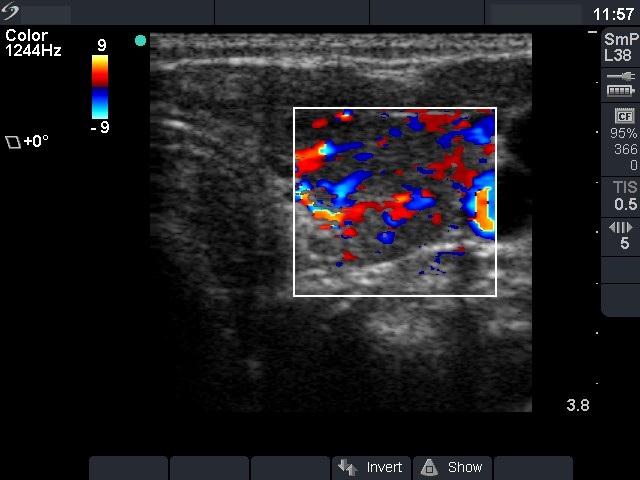
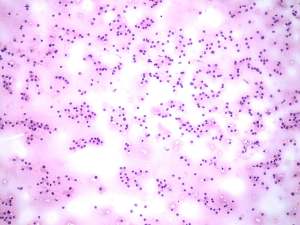
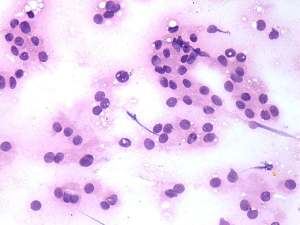
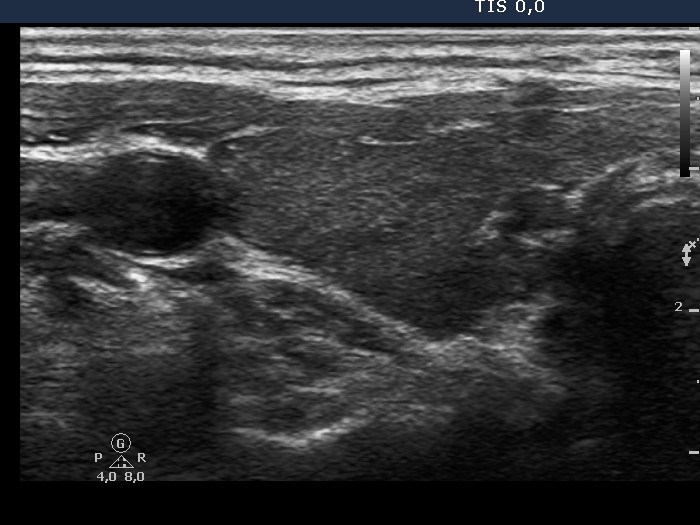
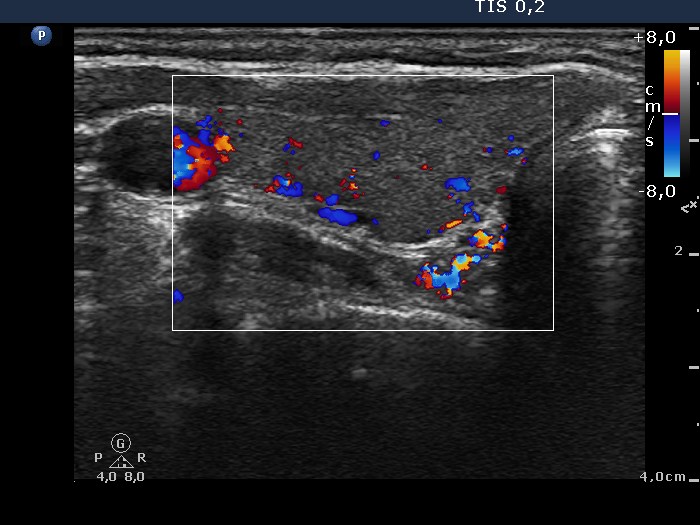
Ultrasonography: the thyroid was hypoechogenic. The vascularization was increased. There was a hyperechogenic discrete lesion with coarse calcification in the central part of the left lobe.Cytology from the hyperechogenic lesion. Benign follicular proliferation with signs of hyperfunction.
Clinical diagnosis: hyperthyroidism caused by Graves-Basedow's disease.
We administered daily 30 mg methimazole to the patient.
Follow-up examination 3 months later (third row):
Clinical presentation: the patient was well, her complaints had resolved.
Functional state: subclinical hyperthyroidism on daily 10 mg methimazole with undetectable TSH, FT4 12.9 pM/L.
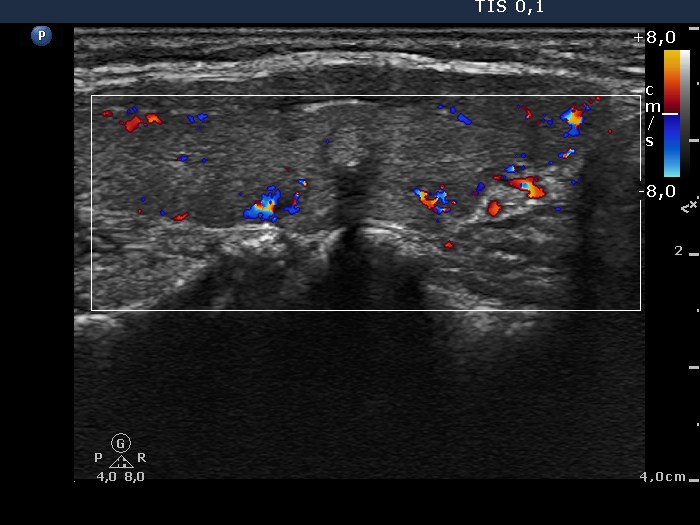
Ultrasonography: the echo structure of the thyroid became moderately hypoechogenic. The vascularization has not changed.
The dose of the methimazole was reduced to daily 10 mg.
Follow-up examination 6 months after initial examination (fourth row):
Clinical data: the patient was well.
Functional state: euthyroidism with TSH-level 2.93 mIU/L, FT4 13.9 pM/L.
Ultrasonography: the size of the thyroid had decreased. The echo structure of the thyroid became minimally hypoechogenic. The vascularization has not changed.
The dose of the methimazolel was not changed.