
|
|
Graves' disease - Case 9.
|
|










Clinical data: A 26-year-old man requested a second opinion. He was treated for Graves' hyperthyroidism for a year. The hyperthyroidism recurred three months after discontinuation of thyrostatic therapy. TSAb was measured and resulted in 15 U/mL on the first examination. Except for repeat TSH and FT4 measurements, no other tests were performed.
Palpation: a firm nodule in the lower pole of the right lobe.
Results of blood tests: hyperthyroidism (TSH undetectable, FT4 29.8 pM/L).
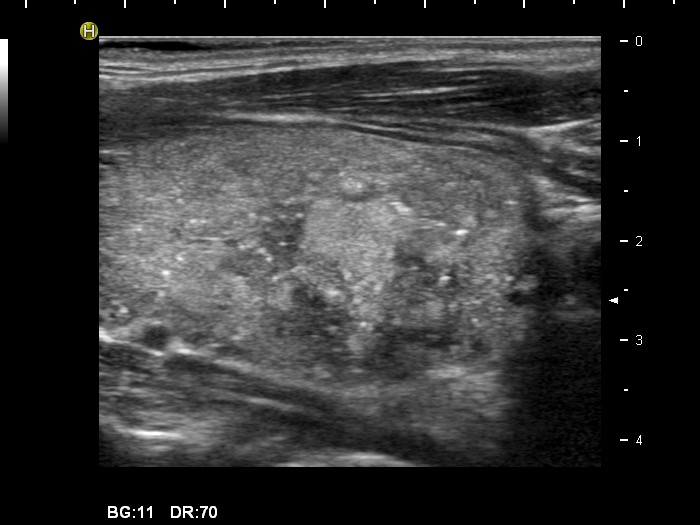
Ultrasonography: The thyroid was echonormal with small minimally hypoechogenic areas. There was a hyperechogenic, inhomogeneous nodule in the lower part of the left lobe. The nodule presented microcalcifications and coarse calcifications, as well. The intranodular blood flow was irregularly increased. The maximal diameter of the nodule was 29 mm.
We indicated scintigraphy which demonstrated a "cold" nodule in the right thyroid.
Cytology was performed from the hyperechogenic nodule.
Cytological diagnosis: the possibility of a papillary cancer cannot be excluded.
Surgery was advised.
Histopathology: Diffuse goiter corresponding to Graves' disease. Benign hyperplastic nodules according to the nodule in the right lobe.
Comments:
-
Thyroid ultrasonography had to be performed at first examination. A young patient with a 3 cm nodule has a very low chance to avoid surgery later in the course of his life. If he has a hyperthyroidism, the chance to avoid surgery is minimal.
-
The sonographic pattern at the time of the recurrent hyperthyroidism is less specific because the evolution of the classical hypoechogenicity requires months, and in the event of a recurrence, the patients visit the doctor sooner than at the first presentation of the disease.
-
By reviewing the smear, we did not change our original report. We have to accept that in certain cases of atypia the cytology cannot exclude the malignancy with enough safety.