
|
|
Chronic lymphocytic thyroiditis - Case 24.
|
|









Clinical data: a 36-year-old woman was referred for an evaluation of hyperthyroidism. She had typical complaints for 2 months, including 6 kg weight loss. Her thyroid was tender. She presented mild degree of thyroid associated ophthalmopathy.
Palpation: both thyroids were firm and tender on palpation.
Functional state: hyperthyroidism with undetectable TSH, FT4 37.9, FT3 9.41 pM/L.
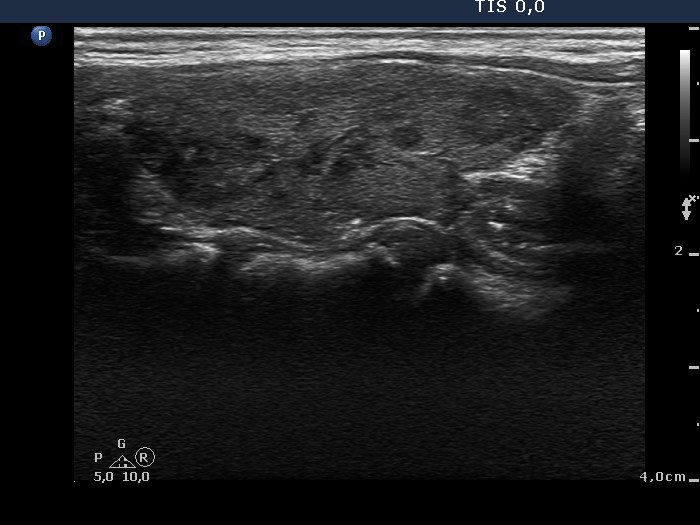
Ultrasonography: the thyroids were composed of hypoechogenic areas not fitting a nodule. The vascularization was significantly increased in the right, while decreased in the left lobe.
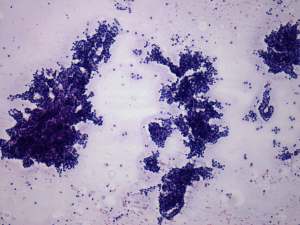
Cytology: benign follicular proliferation.
Thyrostatic was administered, i.e. daily 20 mg methimazole.
Summary of follow-up:
Two weeks later the patient visited us again and was presented with clinical and laboratory signs of hypothyroidism (TSH undetectable, FT4 6 pM/L). The thyrostatic therapy was stopped.
The next visit occurred 2 months later . The patient gained 10 kg in weight, and the hormonal evaluation disclosed severe hypothyroidism with TSH 38.1 mIU/L, FT4 8.1 pM/L. Replacement therapy was started with 75 microgram levo-tiroxine.
One year later the patient was euthyroid and free of complaints on daily 125 microgram levo-tiroxine. TSH was 1.18 mIU/L while FT4 15.2 pM/L.
Comments:
-
This patient had hashitoxicosis at the time of her first visit. Taking the tenderness of the thyroid and the relatively mild hyperthyroid state into account, we considered this possibility despite the increased vascularization on Doppler mode and TAO, but cytological examination did not disclose Hashimoto's thyroiditis.
-
Note the microfollicular proliferation which is not an infrequent finding in the case of Hashimoto's thyroiditis.