
|
|
Chronic lymphocytic thyroiditis - Case 54.
|
|


Clinical data: a 40-year-old woman was referred for a second opinion. She presented hypothyroidism. A hypoechogenic nodule was found on ultrasonography and the result of FNAC was 'follicular cancer with great probability'.
Palpation: no discrete lesion. The whole thyroid was moderately firm.
Results of blood tests: euthyroidism on 75 microgram levo-tiroxin therapy with TSH-level 2.05 mIU/L.
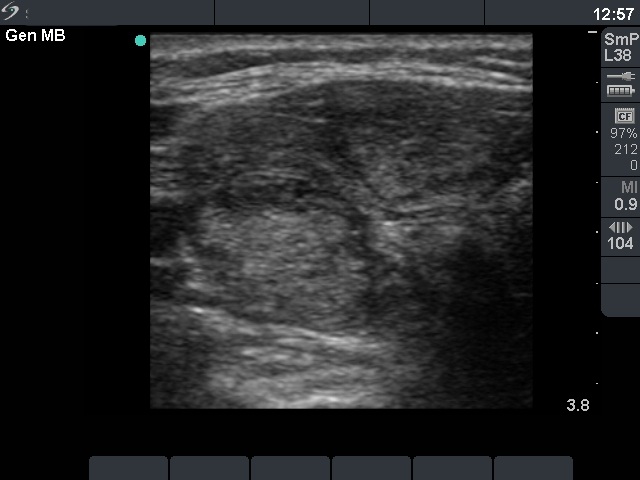
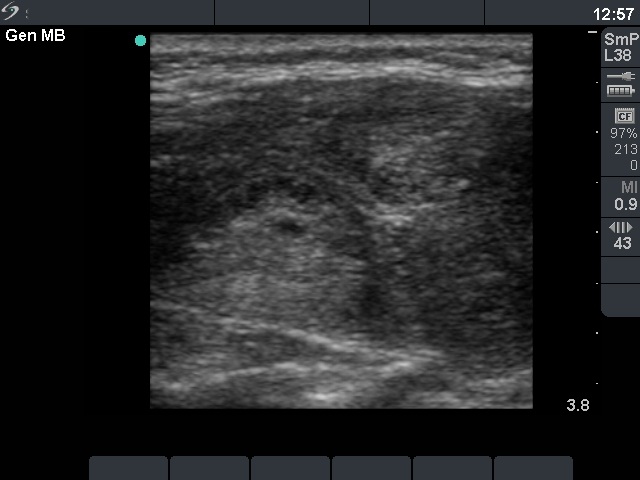
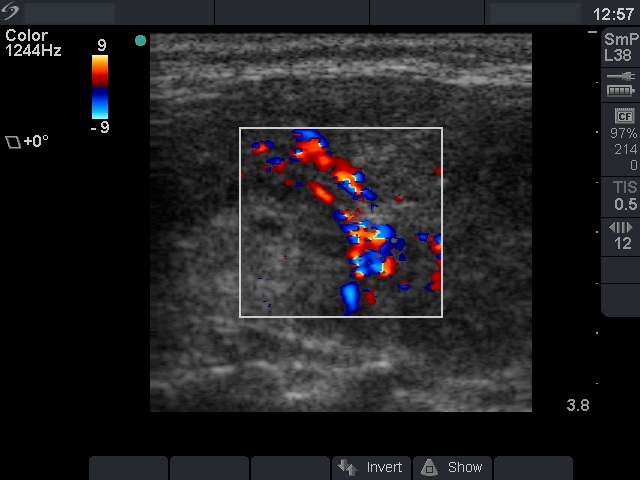
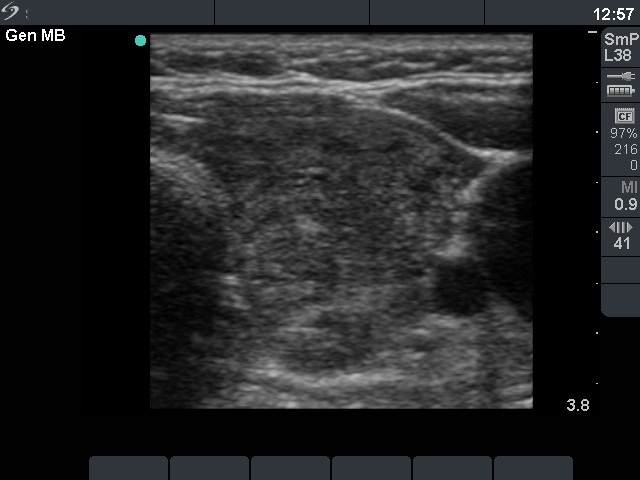
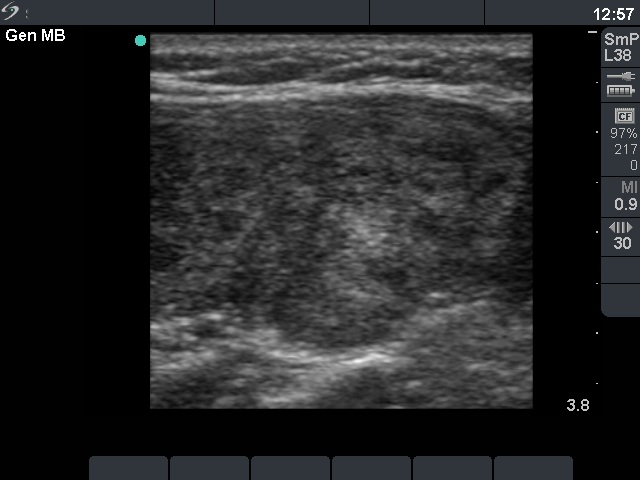
Ultrasonography: the thyroid was hypoechogenic with two well-circumscribed hyperechogenic areas in the right lobe. These were surrounded with a halo and presented perinodular blood flow.
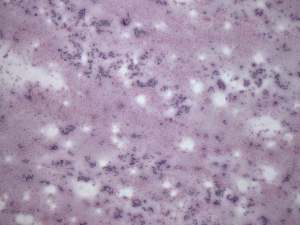
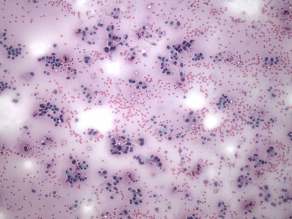
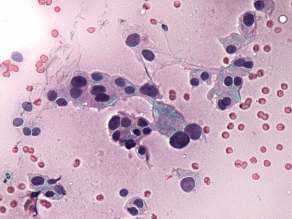
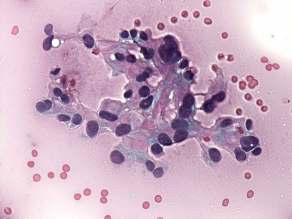
Cytological picture: no colloid in the background. Thyrocytes in small groups, in microfollicles and dissociated. Almost all follicular cells exhibit oxyphilic metaplasia. There were a few foci of nuclear debris but no lymphocytes were present. Note that the follicular cells did not present nucleoli.
Cytological diagnosis: Hürthle-cell tumor.
Histopathology : Hashimoto's thyroiditis without any nodule.
Comment: it was unequivocal that the patient had Hashimoto's thyroiditis. The sonographic picture was equivocal whether the patient had nodule or nodules, too. However, the cytology was more problematic. It became evident after histopathology that the lesion in question was a focus with proliferation of oxyphilic cells. What did we do wrong? I think that such cytological picture itself is almost identical with that seen in a Hürthle-cell tumor. Although there were signs which disfavor the possibility of tumor, we could not exclude the presence of tumor with enough safety. Two minor signs were remarkable: firstly, the presence of nuclear debris which was suspicious for the presence of lymphocytic infiltration even within this lesion ; secondly, the lack of prominent nucleoli decreased the possibility of a Hürthle-cell tumor. The US appearance of the 'nodules' were remarkable. In contrast with a real nodule, these were irregular. Circumscribed areas were also found in the left lobe. Moreover, a follicular tumor is solitary in most cases.
Summary: we missed the combination of the cytological and US findings. If we had put these findings together, it would have been enough to suggest follow-up instead of surgery.