
|
|
Chronic lymphocytic thyroiditis - Case 55.
|
|







Clinical data: a 28-year-old woman was referred for an evaluation of clinical signs of hyperthyroidism.
Palpation: no abnormality.
Functional state: moderate degree of hyperthyroidism (TSH below 0.01 mIU/L, FT4 38.1 pM/L, FT3 8.93 pM/L). TSAb level was not decisive: 2.1 U/L (normal value below 1.5), anti-TPO 203 U/mL.
Ultrasonography: both thyroids were hypoechogenic, inhomogeneous without circumscribed lesions fitting to nodule. The vascularization was increased.
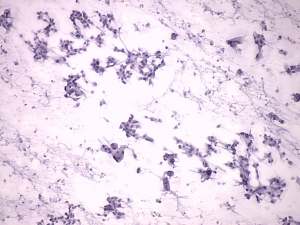
Cytological picture: no colloid in the background. Hürthle-cells were dissociated and in non-specific cell groups, forming multinucleated giant cells. Several nuclear inclusions could be observed. There were only a few lymphocytes on the smear.
Combined ultrasonographic-cytological diagnosis: benign Hashimoto's thyroiditis (although the cytological pattern alone would be sufficient to raise the possibility of papillary cancer).
We did not administer any therapy because the whole picture fitted to hashitoxicosis. The elevated hormone-levels turned to normal in the follow-up examinations and 8 months later the patient became hypothyroid. The dramatic turn occurred when the patient moved to the USA and consulted her medical reports with an endocrinologist who read the details of my original cytological report: 'oxyphilic metaplasia', 'inclusions' - he had doubt about the FNAC diagnosis and initiated a reevaluation by a pathologist in his institute. I sent the smears to him. The reevaluated FNAC diagnosis resulted in the suspicion of papillary cancer and the patient underwent surgery.
Histopathological diagnosis: the entire thyroid was processed and no tumor focus was found. Benign Hashimoto's thyroiditis.
Comment: the FNAC was performed not because of oncological reasons. The sonographic picture including the presence of circumscribed areas was absolutely consistent with an autoimmune thyroid disease. The aspiration was performed to decide whether the elevated hormone levels were caused by an active hormone-producing disorder i.e. Graves disease or were caused by the destruction of a thyroiditis. Nevertheless, the cytological pattern itself would be enough to raise the possibility of a papillary cancer. Theoretically, it was also possible that we had aspirated papillary cancer without discrete echo abnormality. All in all, it was possible with a chance one to a billion.
I had 10 such cases but fortunately only this patient moved to the US. Fortunately, for those cytopathologists who analyse this smear, this patient underwent surgery and and we obtained clear-cut evidence, that this cytological pattern only imitated papillary cancer and it was in fact a benign Hashimoto's thyroiditis.
So it is very important to keep in mind that Hashimoto's thyroiditis may imitate papillary cancer. In equivocal cases, the reevaluation the smear and ultrasonography may prevent the patient from unnecessary surgery.