
|
|
Chronic lymphocytic thyroiditis - Case 82.
|
|










Clinical presentation: a 47-year-old woman requested a second opinion. She was treated for hypothyroidism for 3 years. An ultrasonography was performed on the request of the patient. Aspiration cytology resulted in oxyphilic variant of papillary carcinoma.
Palpation: the right lobe was firm on palpable. No discrete lesion could be palpated.
Hormonal investigation: resulted in minimally elevated TSH-level (4.38 mIU/L) on daily 87.5 microgram levothyroxin.
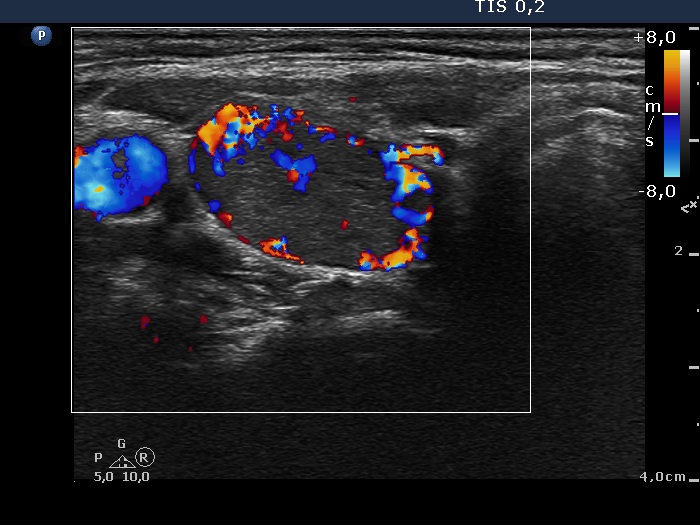
Ultrasonography: the thyroids were hypoechogenic. There was a hypoechogenic lesion in the upper dorso-medial part of the right lobe. The lesion displayed halo sign and a combined type 2 and type 3 vascular pattern. The borders of the lesion were not regular geometrical. The thickness of the surrounding hypoechogenic rim was varying.
Cytological diagnosis: Hashimoto's thyroiditis.
Combined clinical-ultrasound-cytological diagnosis: Hashimoto's thyroiditis with the possibility of oxyphilic variant of follicular tumor with the estimated risk of carcinoma not greater than 2%.
Taking the previous and our results into account we advised lobectomy.
Histopathology disclosed Hashimoto's thyroiditis and no nodule.
Comments.
-
The ultrasound presentation of the lesion highly resembles that of a nodule. Nevertheless, the uneven surface of the lesion and the varying thickness of the hypoechogenic rim surrounding the lesion are arguments against the possibility being the lesion a nodule in a pathological sense. Nevertheless, these arguments are absolutely not decisive but they had to be considered.
-
The cytological pattern is also remarkable. The presence of intranuclear holes led to the false diagnosis. These figures do not fit a typical inclusion. The ratio of oxyphilic cells to lymphocytes is unusually high, therefore an oxyphilic tumor has to be considered. On the other hand, follicular cells lack prominent nucleoli and a tendency to dissociate.
-
Taking the sonographic and cytological preenetation into account we gave the final diagnosis of Hashimoto's thyroiditis. Naturally, a positive cytology cannot be eliminated by a negative one. Therefore the patient had to be operated on, but on the result of the second investigation instead of total thyroidectomy only lobectomy was performed.