
|
|
Chronic lymphocytic thyroiditis - Case 10.
|
|







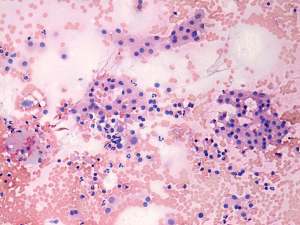

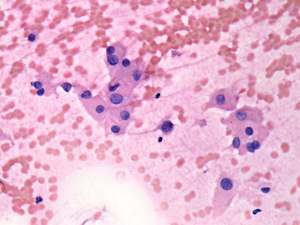



First examination (1st and 2nd rows of images):
Clinical presentation: a 39-year-old woman requested a second opinion. She was referred for an evaluation of hyperthyroidism (TSH undetectable, FT4 39.3 pM/L) 2 weeks prior the present examination. Daily 20 mg methimazole therapy was advised but the patient did not start with the thyrostatic therapy. She lost 6 kg in weight and had palpitation.
Palpation : no abnormality.
Functional state: moderate degree of hyperthyroidism with TSH 0.01 mIU/L, FT4 46.3 pM/L.
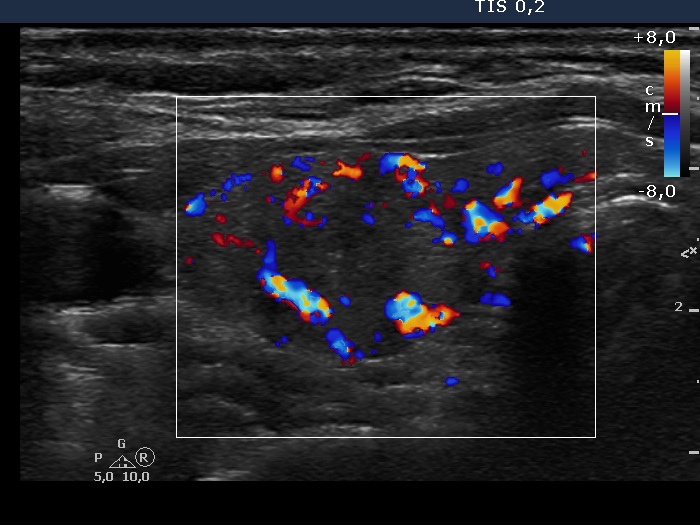
Ultrasonography: around 40% of the thyroids were hypoechogenic. The vascularization was decreased.
FNAC disclosed Hashimoto's thyroiditis.
We performed TsAb test which proved to be elevated: 12 U/L (normal value below 1.5). Anti-TPO 102 U/mL.
Final diagnosis: Hashimoto's thyroiditis. Hashitoxicosis with great probability. Taking all circumstances into account, we advised not to treat the elevated hormone-levels.
Follow-up examination 4 weeks later:
Clinical presentation: the patient felt better, she gained 3 kg back.
Results of blood tests: TSH undetectable, FT4 15.5 pM/L.
Follow-up examination 3 month later:
Results of blood tests: TSH 6.08 pM/l, FT4 9.06 pM/L.
Follow-up examination another 3 month later:
Results of blood tests: TSH 3.77 mIU/l, FT4 12.1 pM/L.
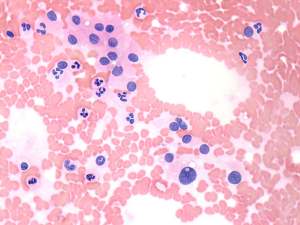
Follow-up examination 31 months after the initial investigation (3rd row of images):
Clinical presentation: the patient had no complaints.
Palpation: no abnormality.
Functional state: TSH 9.43 mIU/L, FT4 10.0 pM/L.
Ultrasonography: the thyroid was larger compared with the initial examination. Except for the vascularization became increased, the sonographic pattern remained unchanged.
Replacement therapy was started.
Comments.
-
We think that the performance of ultrasound is mandatory in the event of moderate degree of hyperthyroidism without thyroid associated orbitopathy. We have found that decreased vascularization on ultrasound is a stronger argument against active hormone-producing process than elevated TsAB for that. Moreover, the performance of FNAC is very useful in such cases and may decide the differential diagnostic problem.
-
The patient presented a typical course of the so-called hashitoxicosis. A hyperthyroid phase was followed by a hypothyroid phase and months later the thyroid spontaneously became euthyroid.