
|
|
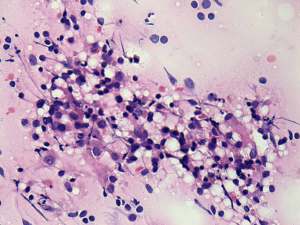
Chronic lymphocytic thyroiditis - Case 11.
|
|






Clinical presentation: a 37-year-old woman was referred for aspiration cytology. She was diagnosed with having hypothyroidism and a suspicious nodule was found on ultrasound.
Palpation: no abnormality.
Functional state: hypothyroidism with TSH 13.2 mIU/L, FT4 8.09 pM/L.
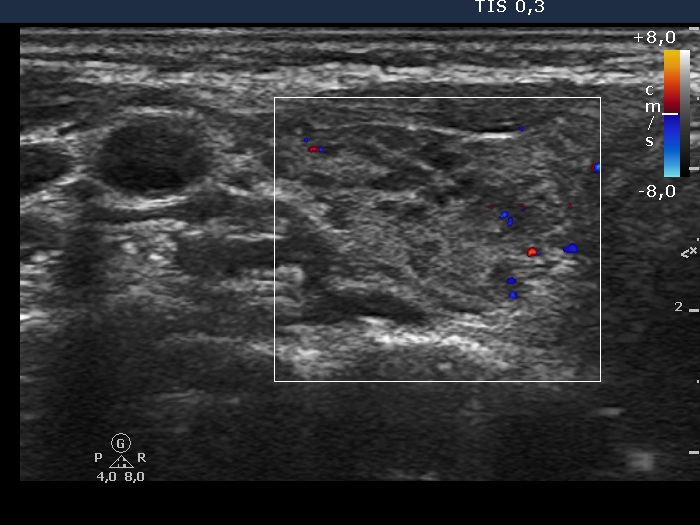
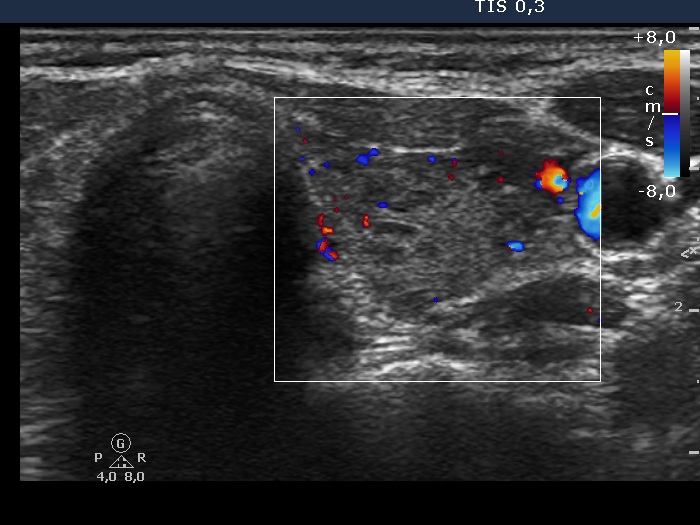
Ultrasonography: the thyroid was echonormal with many hypoechogenic areas of various sizes. The echogenicity index was around 30%. We found no suspicious lesions, the hypoechogenic area in question was located in the ventrolateral part of the thyroid. None of the hypoechogenic areas fit nodule, these were in fact more active foci of lymphocytic thyroiditis.
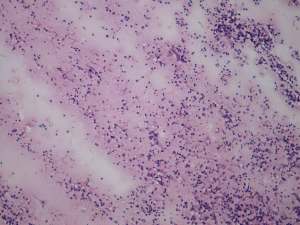
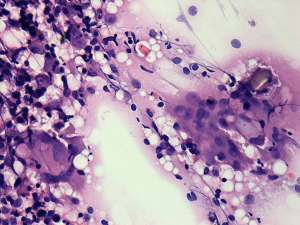
FNAC: disclosed Hashimoto's thyroiditis.
Histopathology: disclosed Hashimoto's thyroiditis without any nodule.
Comment: the presence of multinucleated giant cells in the case of a thyroiditis argue for de Quervain's thyroiditis. Nevertheless, the ultrasound pattern including the normal vascularization excluded this possibility.