
|
|
Follicular adenoma - Case 34.
|
|







Clinical data: a 40-year-old woman requested an evaluation for weight gain.
Palpation: the thyroids were firm, and a nodule was palpable in the left lobe.
Hormonal examination: indicated subclinical hypothyroidism with TSH 8.01 mIU/L, FT4 10.9 pM/L.
Ultrasonography: the thyroid was hypoechogenic. There was an echonormal nodule with a halo sign in the right lobe. Type 2 vascular pattern, i.e. perinodular blood flow was detected.
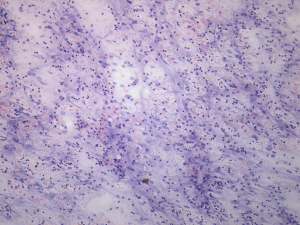
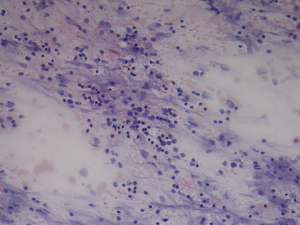
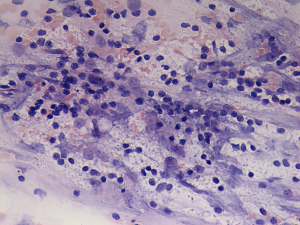
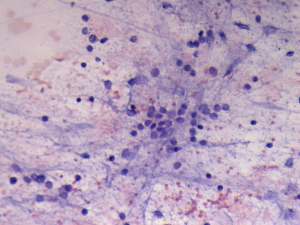
Cytological picture: there is no colloid in the background. Heterogeneous lymphoid population was the predominate cells type. There were only scattered number of follicular cells on the smear. They occurred dispersed and forming micro- and normofollicles. The cytological pattern corresponded to Hashimoto's thyroiditis.
Combined clinical-sonographic-cytological diagnosis: subclinical hypothyroidism caused by Hashimoto's thyroiditis. Suspicion of a follicular tumor with less than the average risk for malignancy.
We offered regular follow-up investigation instead of surgery because there was no atypia on the smear and the nodule was echonormal. This combination means that the risk of malignancy is less than 1:100. The patient was operated 2 years later for unknown reasons.
Histopathological diagnosis: microfollicular adenoma. Hashimoto's thyroiditis in the extranodular part.