
|
|
Follicular adenoma - Case 36.
|
|










Clinical data: A 45-year-old man requested a second opinion. Ha discovered a nodule in the right lobe for 3 months. Evaluation was performed in another institute. FNA was repeatedly not diagnostic. He was told to harbor "thyroid carcinoma with relatively great probability" because the nodule was very hard and presented the so-called starry sky appearance caused by numerous microcalcifications.
Palpation: a hard nodule in the right lobe.
Hormonal examination: euthyroidism with TSH 1.63 mIU/L.
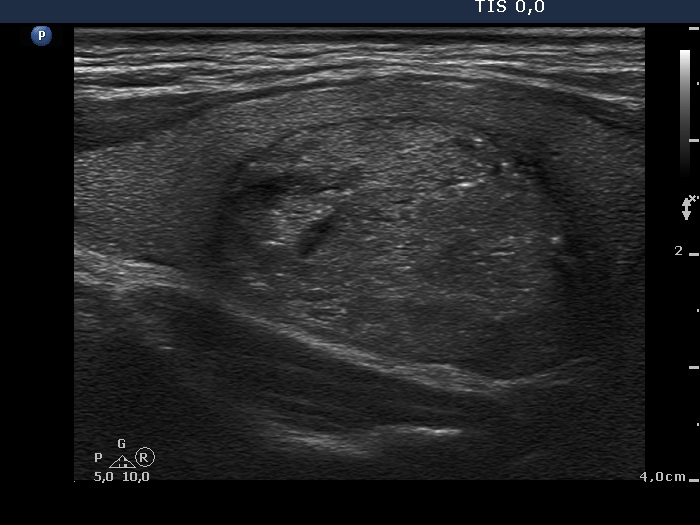
Ultrasonography: The thyroid was echonormal. There was an echonormal nodule presenting hyperechogenic granules and lines. The lesion displayed halo sign and perinodular vascularity.
Cytological picture: There is diffuse colloid in the background. Follicular cells occur predominantly in normofollicles. Thyrocytes present coarsely granular chromatin structure but lack prominent nucleoli.
Combined clinical-sonographic-cytological diagnosis: follicular tumor with great probability but with less than 1% estimated risk of carcinoma.
We offered regular follow-up investigation instead of surgery. Our suggestion was held as inappropriate by the endocrinologist who performed the original evaluation. Total thyroidectomy was advised. The patient phoned me. Considering the previously described situation I did not talk the patient from surgery but I advised lobectomy instead of total thyroidectomy.
Histopathology disclosed follicular adenoma.
Comments.
-
The intranodular hyperechogenic figures were misinterpreted as microcalcifications by the former investigator. They were in fact signs of fibrosis. Fibrosis makes a node very firm.
-
A patient with a follicular tumor has around 3% risk harboring carcinoma in our moderately iodine-deficient region. Therefore, to operate all follicular tumors seems not to be an adequate approach in our country.
- Let's take the available data into account.
- The hard consistency of the nodule was explained by fibrosis - not an argument favoring malignancy.
- The nodule was echonormal - a strong argument against malignancy.
- The cytology and the sonographic presentation proved that the lesion is follicular tumor - without cytological atypia.
- It is a hard situation if two specialists are on diverse options. If one states that the patient harbors malignancy, than the patient has to be send to surgery - not only because of judicial and ethical but also because of self-evident psychological reasons.
The risk of carcinoma is not greater than 1%.