
|
|
Chronic lymphocytic thyroiditis - Case 52.
|
|








Clinical presentation: a 31-year-old woman requested a second opinion. On previous ultrasonography a 'multinodular goiter' was diagnosed with a 'suspicious hypoechogenic nodule with microcalcification'. The result of FNAC was 'Hürthle-cell tumor or Hashimoto's thyroiditis'. She wanted a second investigation before surgery.
Palpation: both thyroids were moderately firm. No nodule could be palpated.
Results of blood tests: euthyroidism with TSH-level 1.71 mIU/L, FT4 14.0 pM/L, anti-TPO < 10 IU/mL.
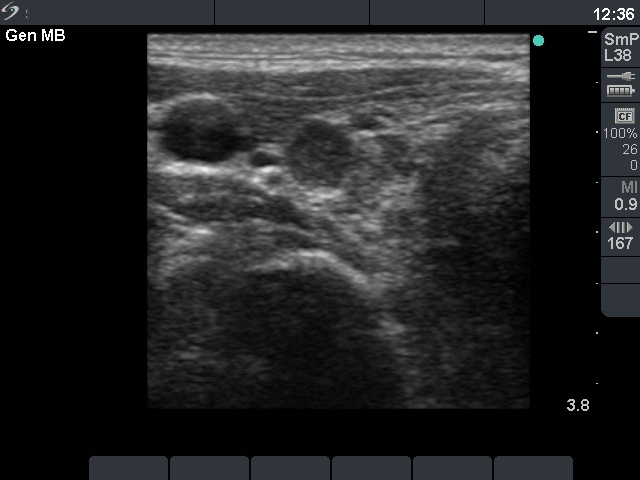
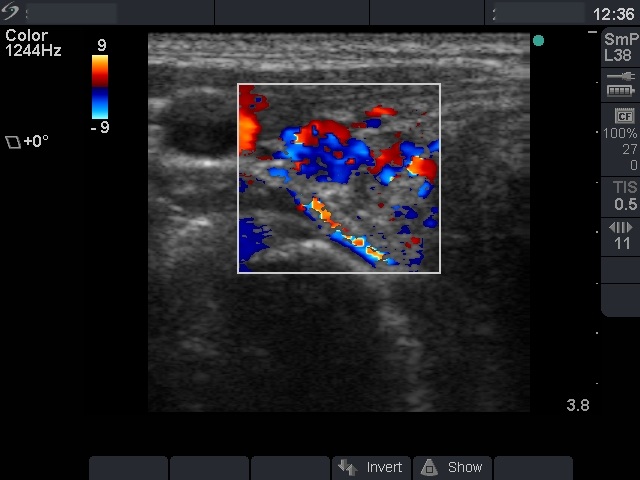
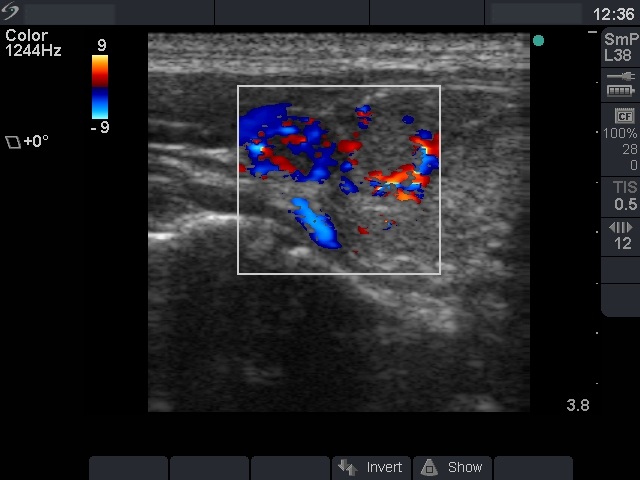
Ultrasonography: the thyroid was composed of small hyperechogenic areas and one hypoechogenic lesion surrounded with a halo. The size of these lesions were between 5 mm and 13 mm. The vascularization was increased within the hypoechogenic lesion in the right lobe. It contained one small hyperechogenic granule.
Cytological picture: no colloid in the background. Loose clusters of oxyphilic cells were mixed with lymphocytes. The Hürthle-cells had fine chromatin structure, most of them did not contain prominent nucleoli. Although the possibility of a Hürthle-cell tumor could not be fully excluded, it's probability was relatively low.
Combined ultrasonographic-cytological diagnosis: benign Hashimoto's thyroiditis.
The patient had great fear because of the first diagnosis and went on operation.
Histopathology: benign Hashimoto's thyroiditis with no nodule.
Comments.
-
The US pattern was very specific for the so-called micronodular form of Hashimoto's. In this case the lesions were really pseudolobules of the thyroid divided by connective tissue.
-
The sensitivity of the anti-TPO determination is around 90% and significantly worse in euthyroid state of Hashimoto's thyroiditis.
-
A cytopathologist must be aware of his or her responsibility. If the phrase 'tumor' is present on the cytological report, in almost all cases the patient will be operated on.
-
This case is a very good example that proves the need for a new diagnostic system. The sonographic pattern itself is not calming, the cytological picture is not fully calming. However, these together proved that this case is a benign Hashimoto's thyroiditis.