|
|||||||||||||||||||
|
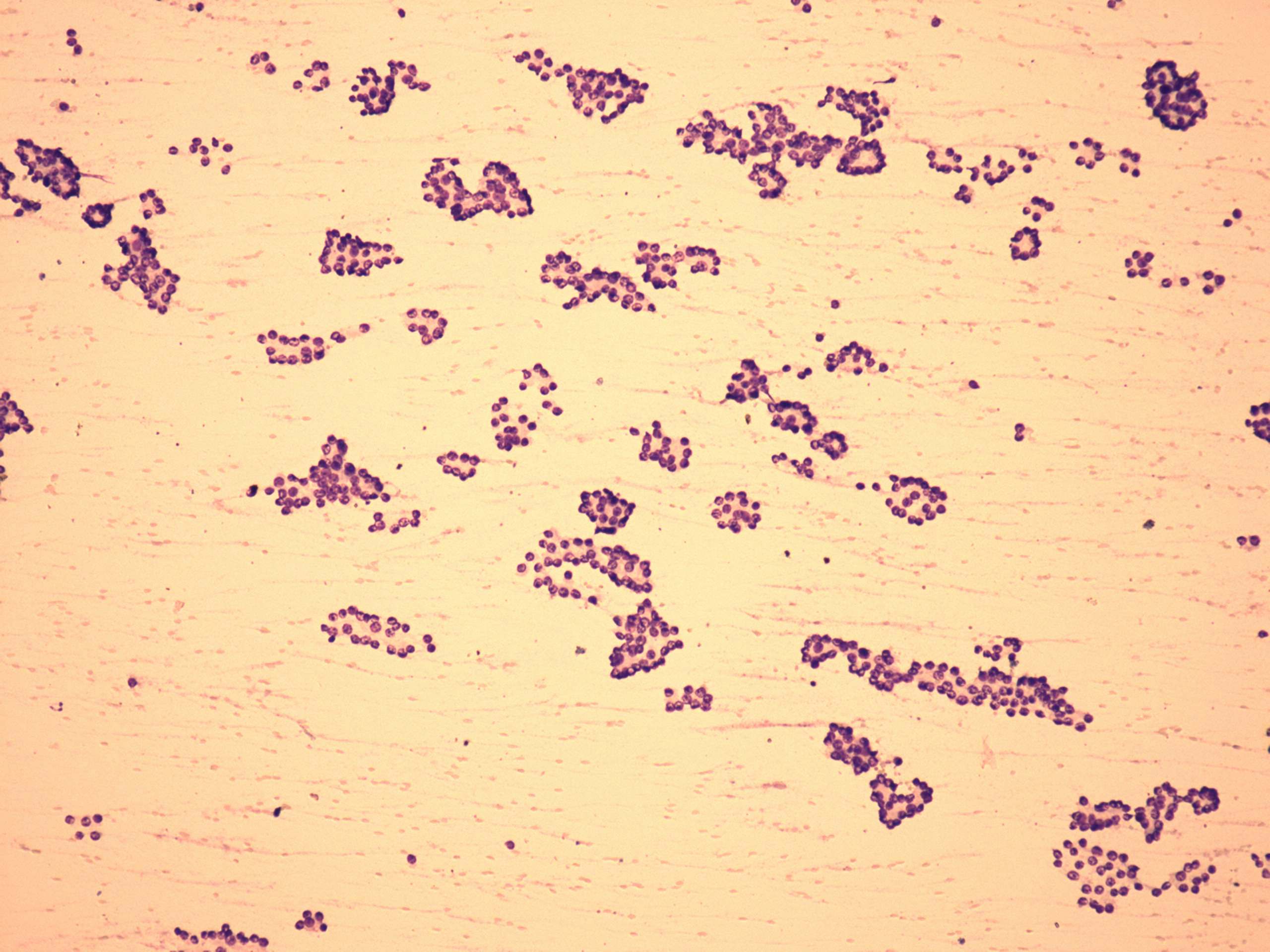
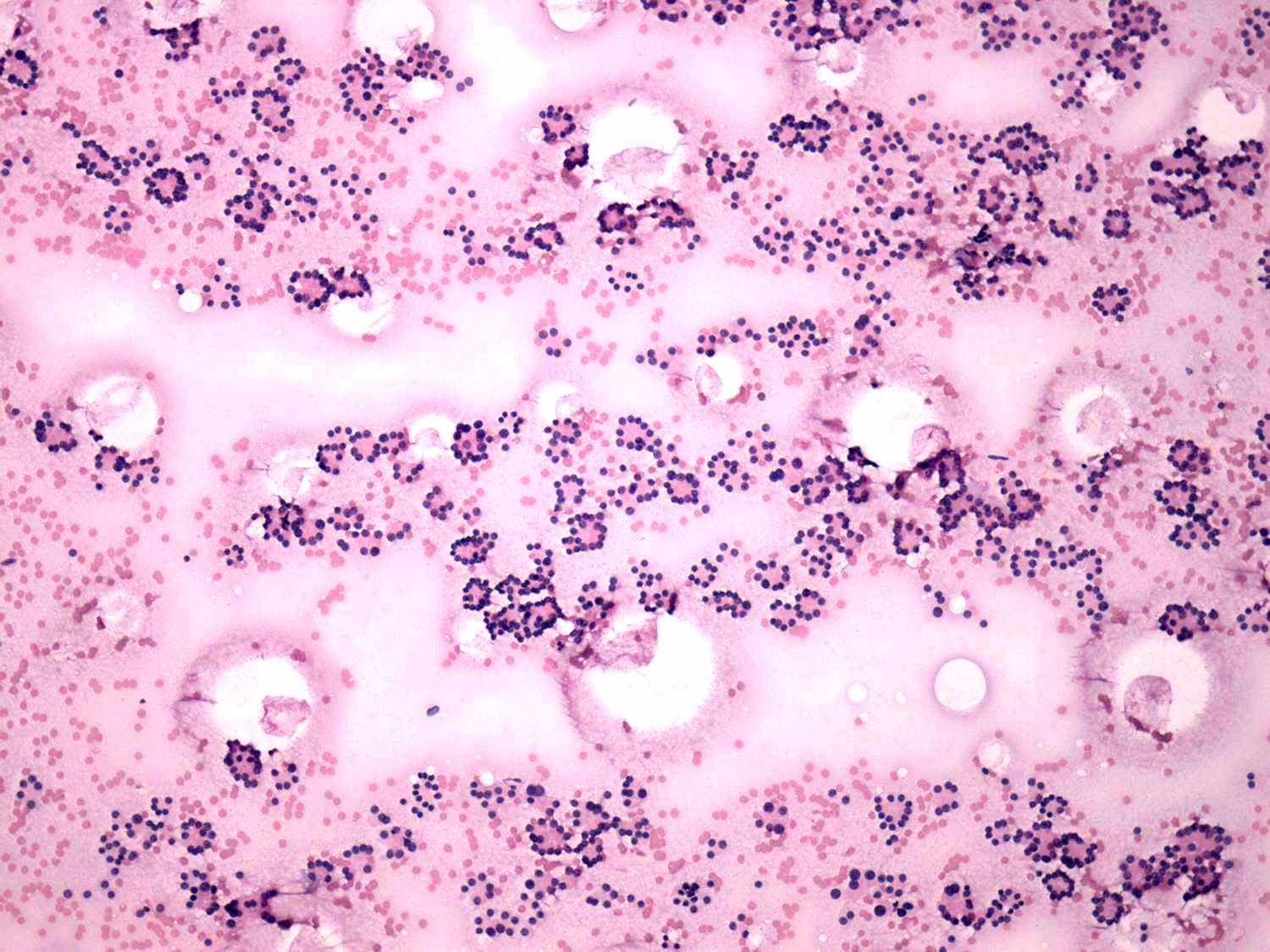
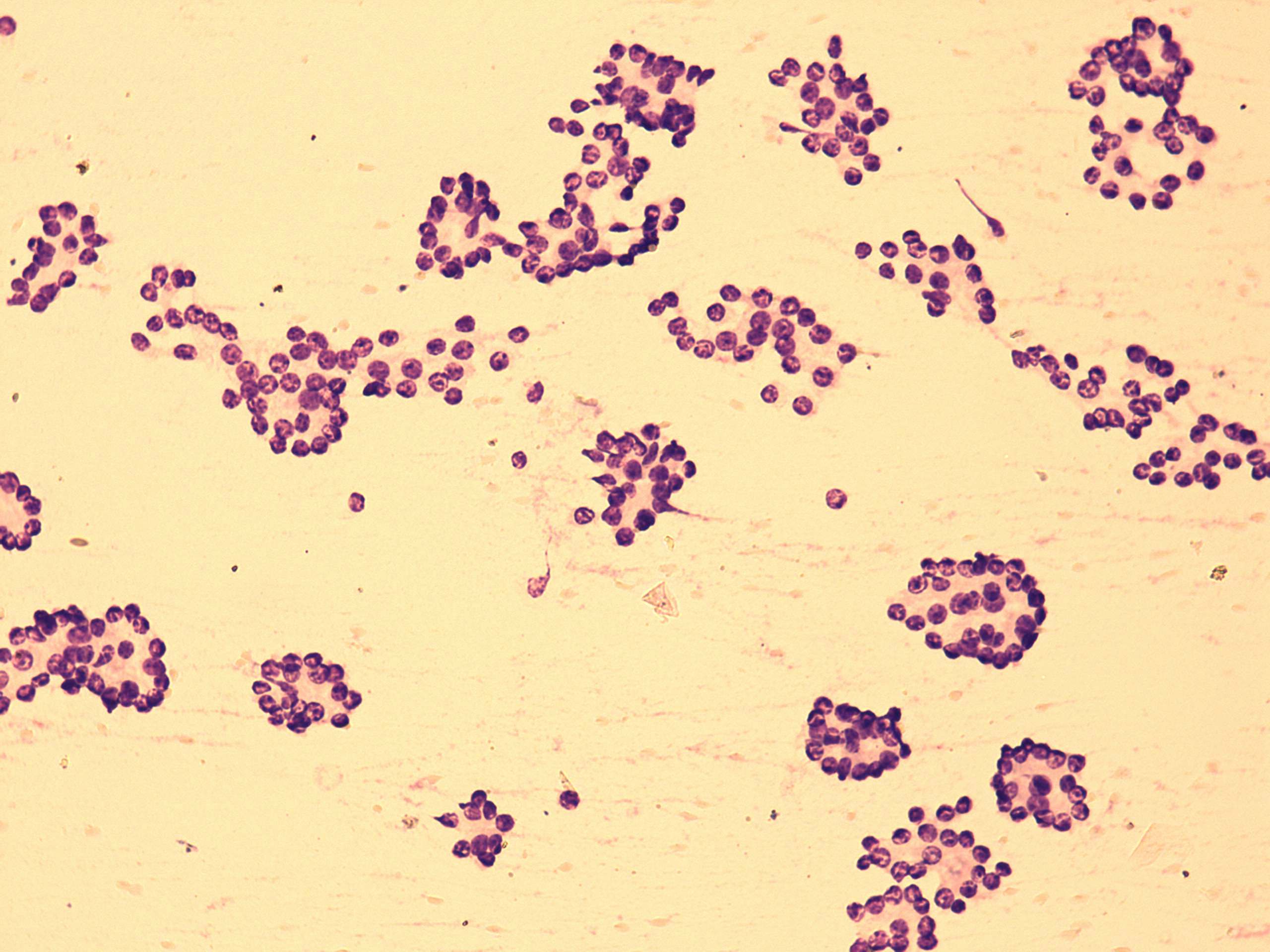
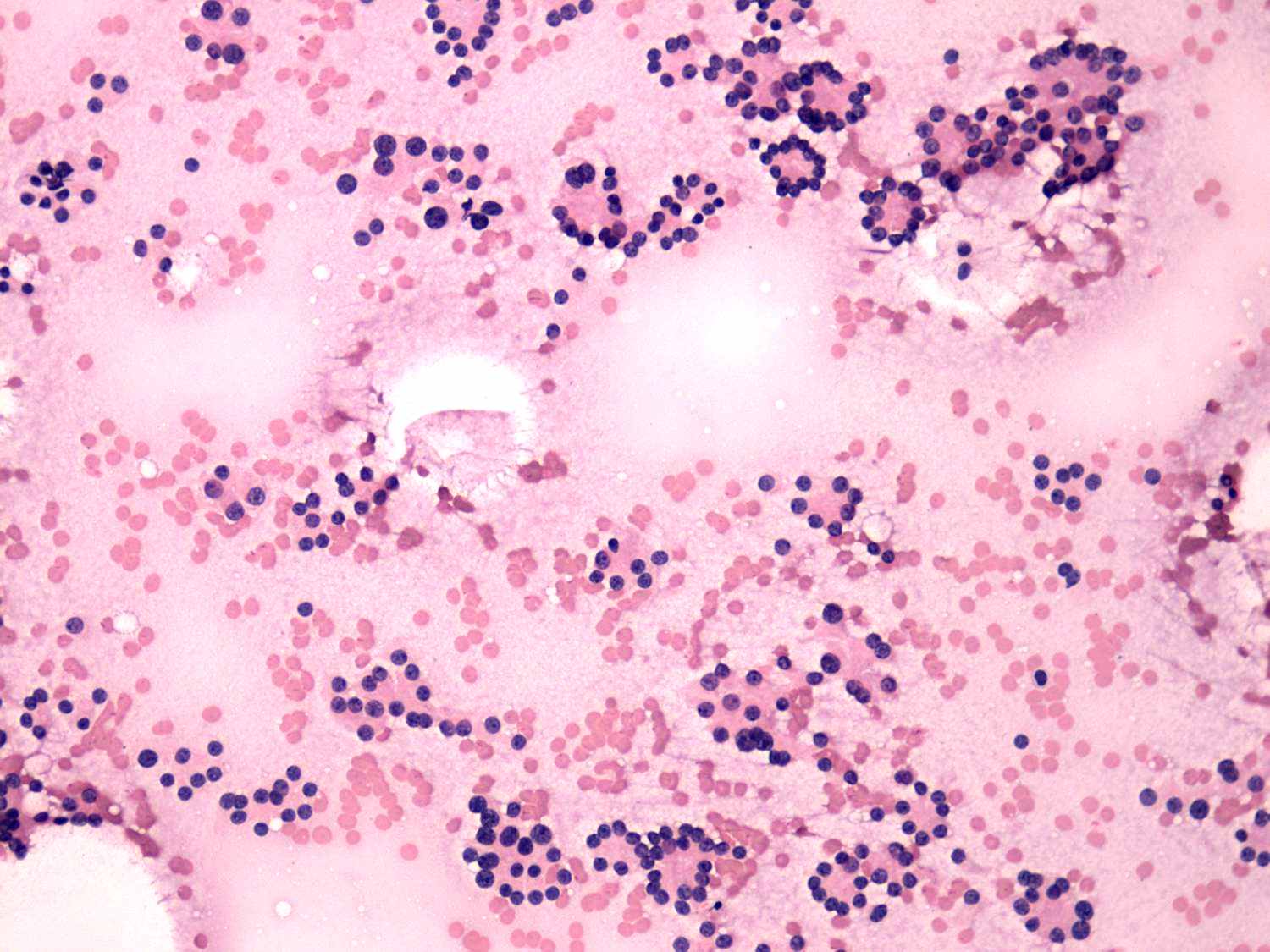
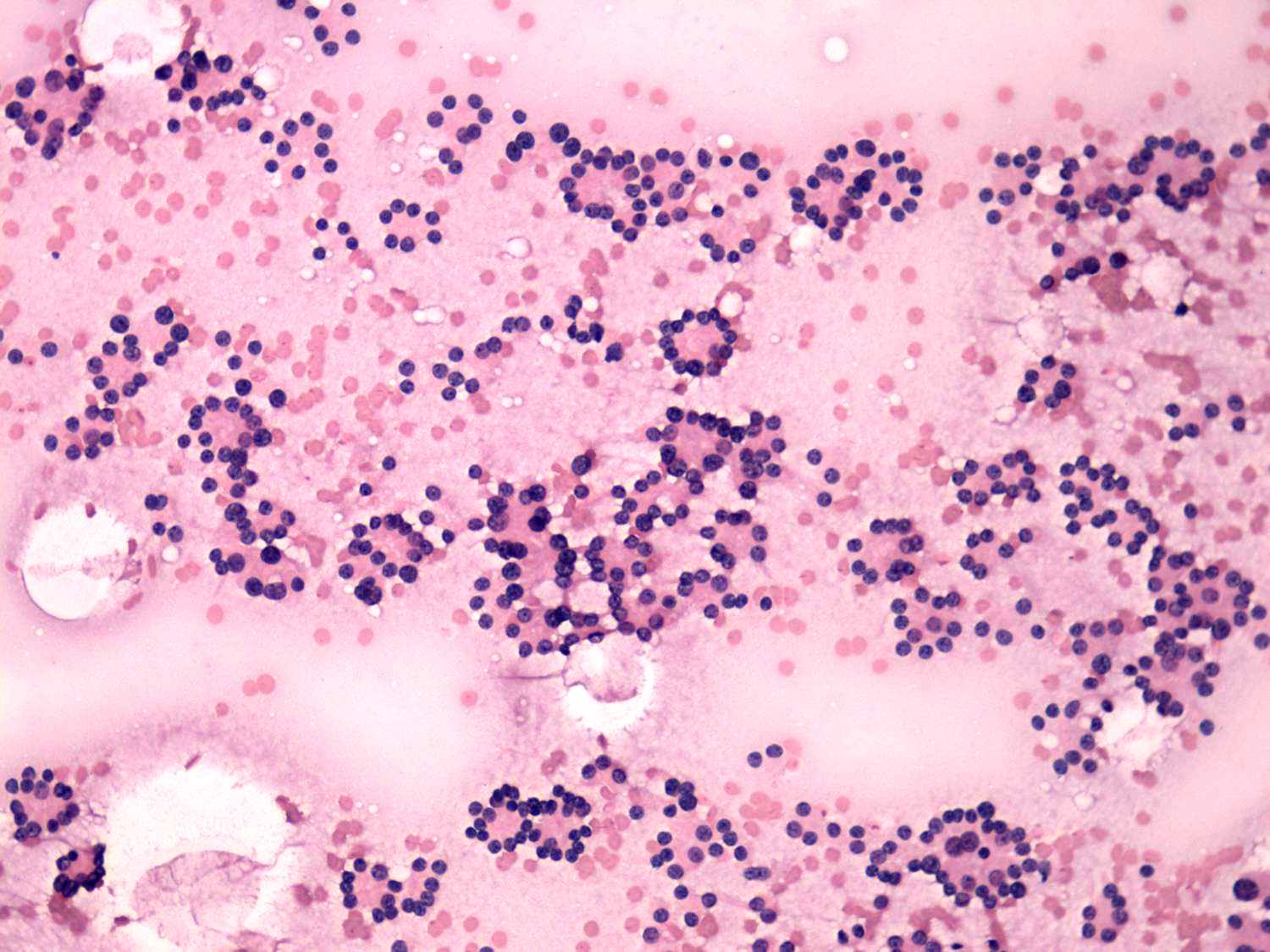
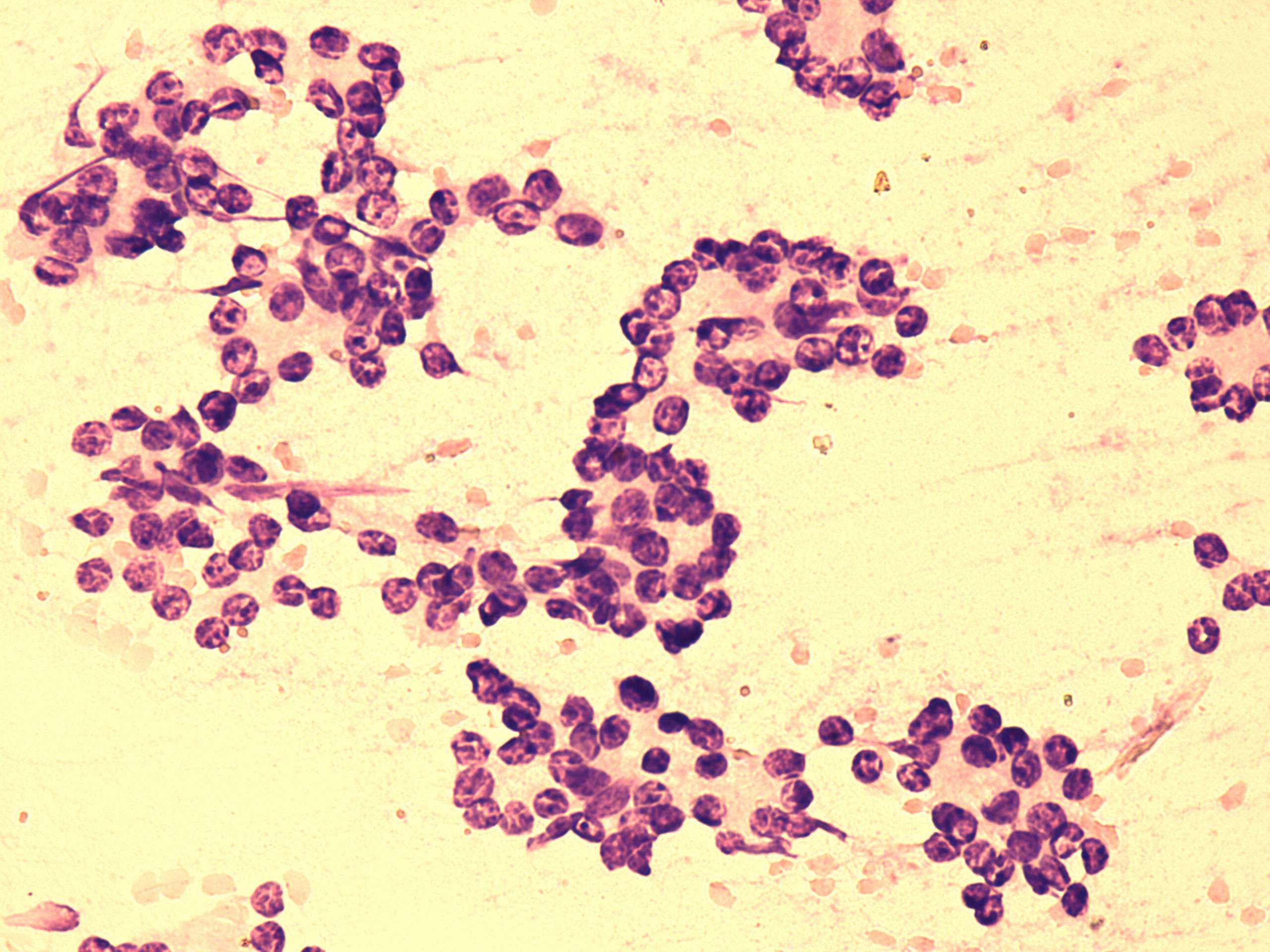
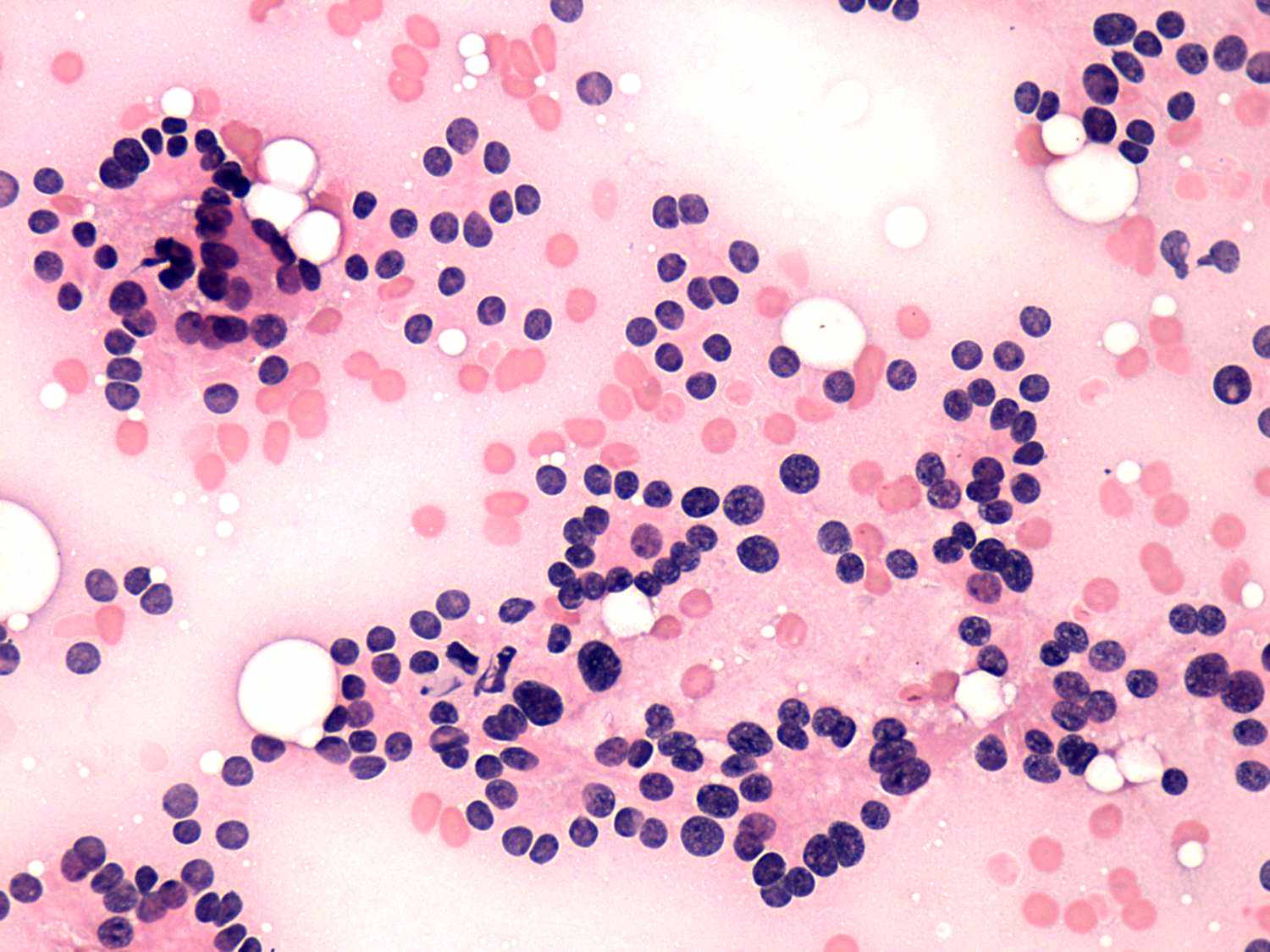
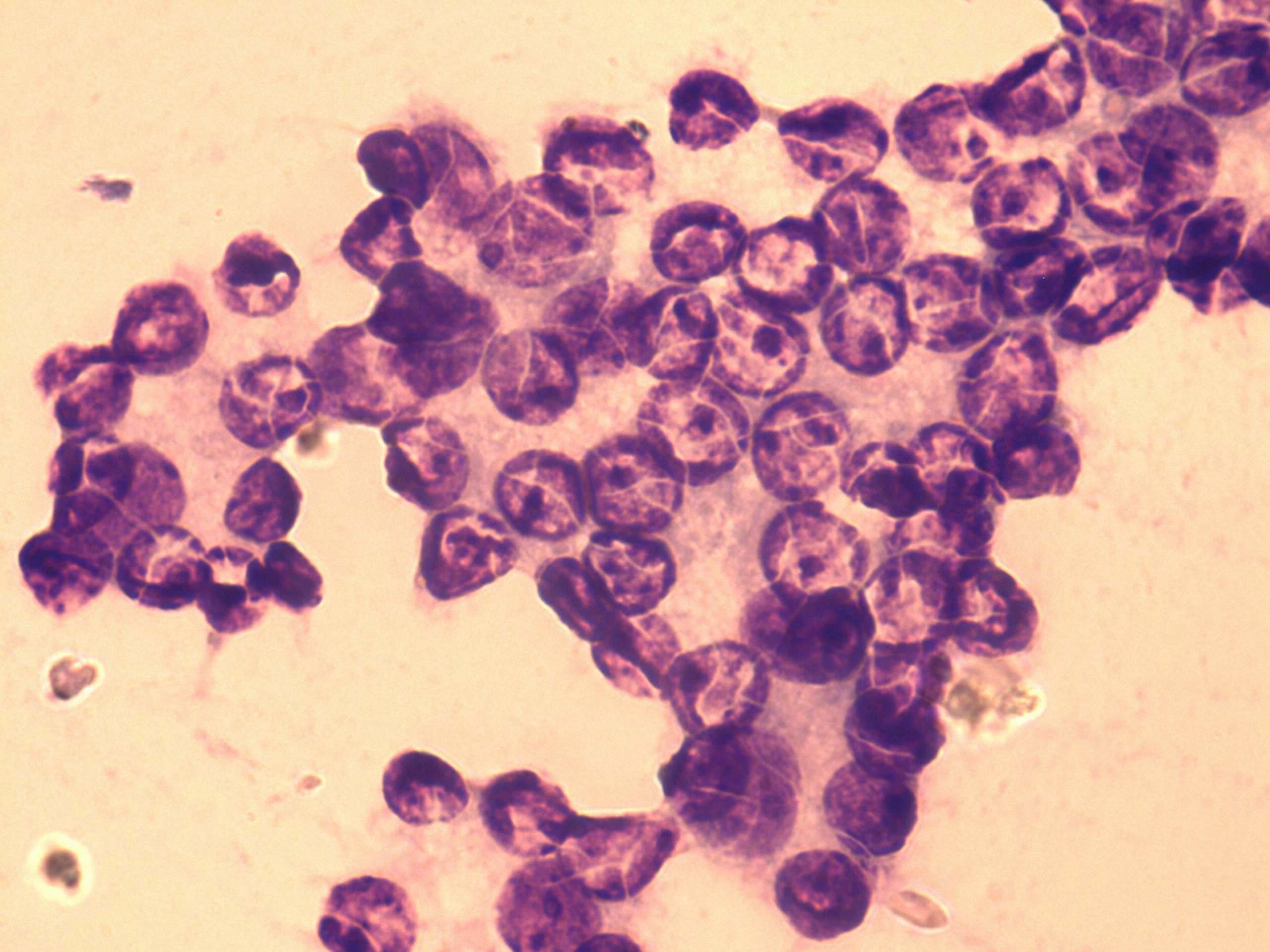
Differential diagnostics of follicular lesions - table 13
|
|||||||||||||||||||
|
|||||||||||||||||||
|
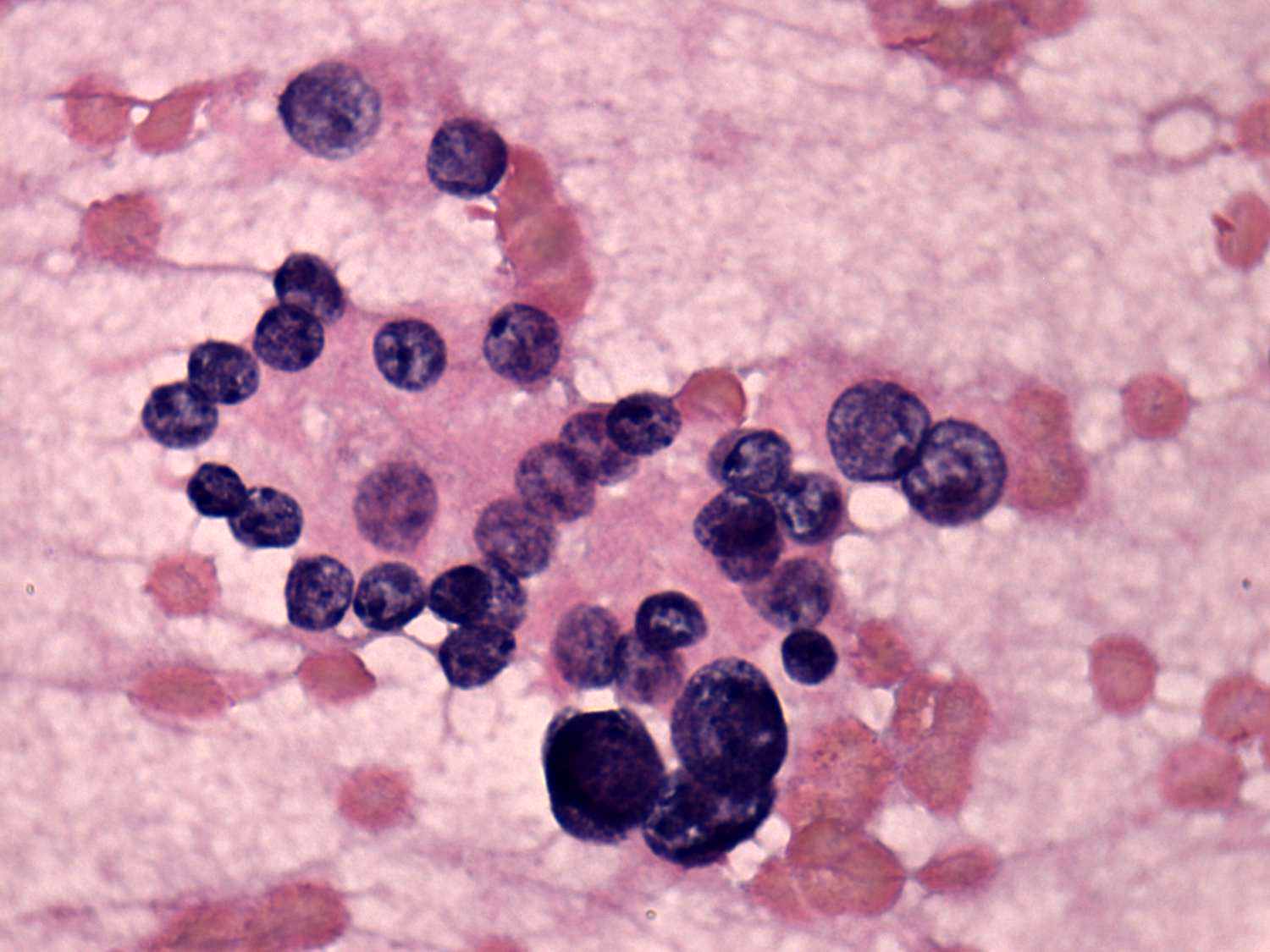
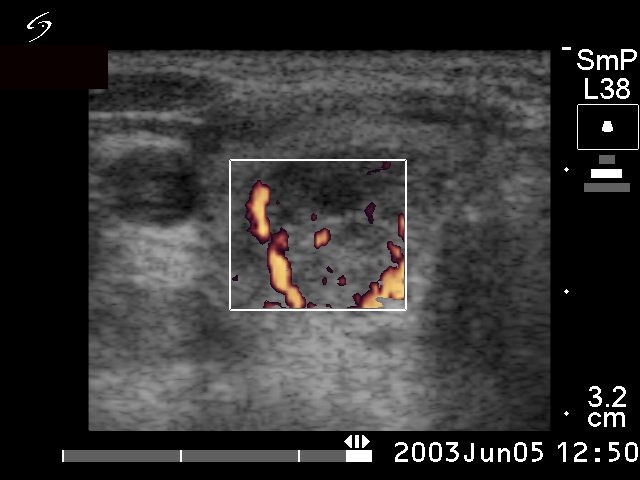
Both cases present a microfollicular proliferation. There were several atypical cells in the right case which increased the likelihood of malignant variant of follicular carcinoma. The ultrasound presentation of the left case is equivocal. A solitary, not regularly geometrical nodule is presented which did not display halo sign. Although there were signs of a perinodular blood flow, most vessels demonstrated in the image run not within the rim of the lesion but run from the border into the lesion. |
|||||||||||||||||||