
|
|
The composition of the nodule - case 1033
|
|



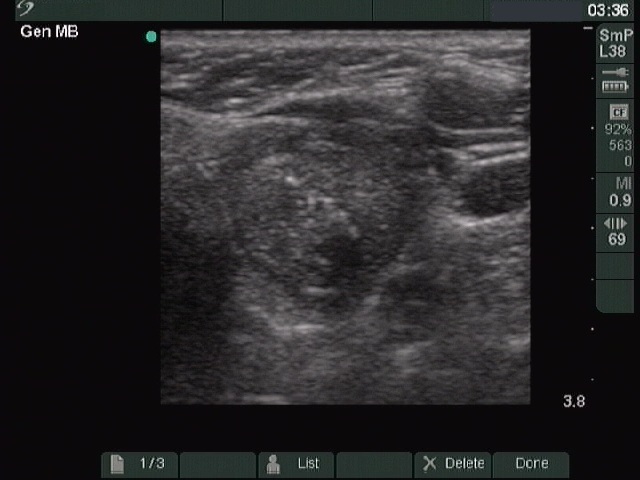


First examination (first row of images):
Clinical presentation: A 56-year-old woman known harboring an autonomously functioning adenoma requested a second opinion. The thyroid problem was known for more than ten years and caused neither hyperthyroidism nor problems. She underwent an ultrasound examination when she was told that her nodule is very suspicious because of the presence of microcalcifications.
Palpation: a not firm nodule in the left lobe.
Result of blood test: TSH 0.34 mIU/L, FT4 17.5 pM/L.
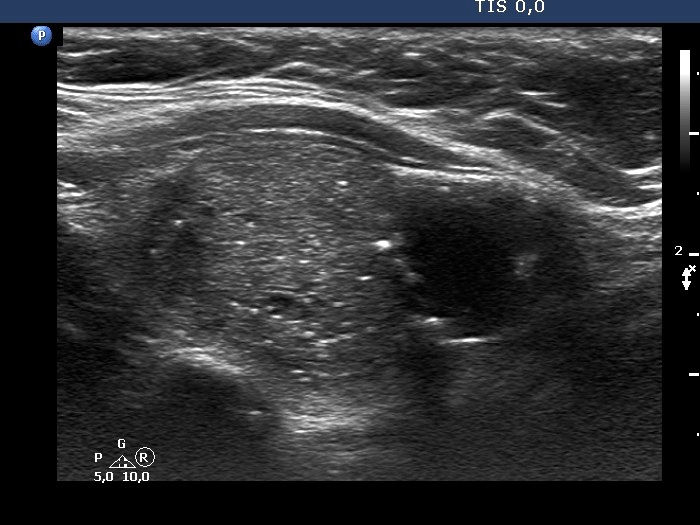
Ultrasonography. The thyroid was echonormal. There was a small hypoechogenic lesion in the right lobe while a nodular area in the left lobe. The latter had an upper, solid part and a lower, cystic part. The former presented echogenic granules and lines.Aspiration cytology was performed from the solid part and resulted in benign lesion.
Suggestion: yearly TSH determination, ultrasound in 4 years.
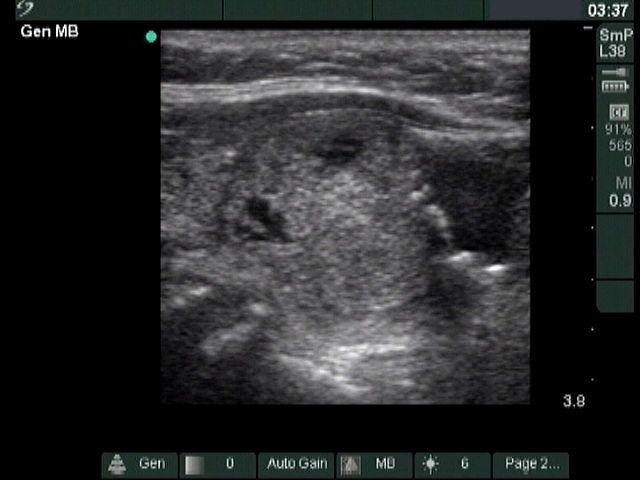
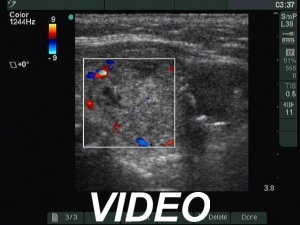
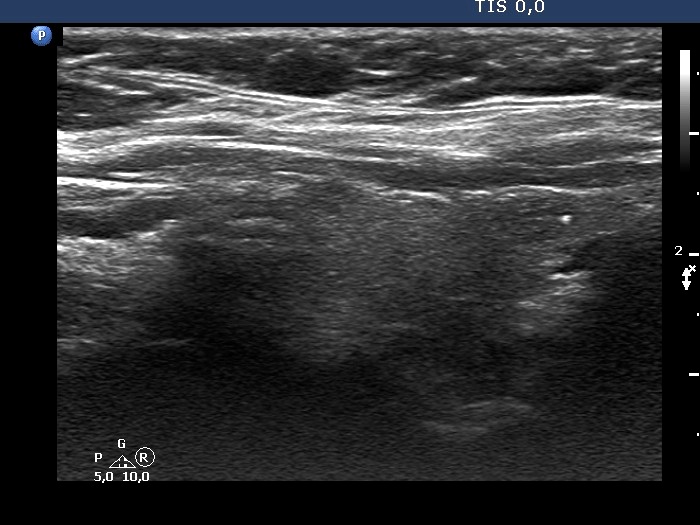
Second examination 7 years later (second and third rows of images):
Clinical presentation: The patient remained euthyroid in the previous years an had no complaints.
Palpation: unchanged.
Result of blood test: TSH 0.34 mIU/L, FT4 14.2 pM/L
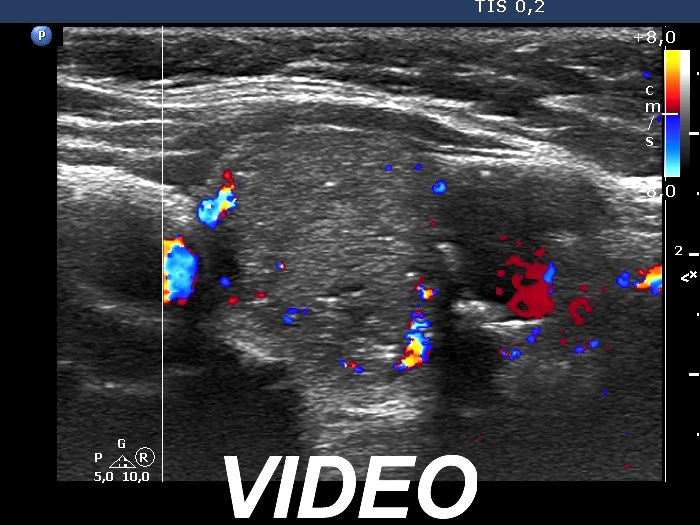
Ultrasonography. The presentation remained unchanged. Using a better ultrasound device, it turned out that the echogenic granules are related to ventral cystic areas. Therefore, these are not microcalcifications, but figures caused by back wall cystic enhancement.Suggestion: yearly TSH determination, ultrasound in 4 years.
Comments.
- Cytology was performed partly on psychological reasons. We can more effectively and permanently reassure a patient if we make cytology compared with a roundabout reasoning.
- The interpretation of the discrete lesions in the left lobe is difficult. I mean that this is a dominantly solitary nodule with a peripheral-type cystic portion. (See the explanation at the images.)