
|
|
Lymphocytic thyroiditis - case 1440
|
|




Clinical data: A 50-year-old woman was referred for an evaluation of a nodular goiter discovered on screening.
Palpation: The whole thyroid was moderately firm. A firm nodule was palpable in the upper pole of the left lobe.
Functional state: euthyroidism (TSH 1.73 mIU/L, FT4 17.0 pM/L, anti-TPO 742 IU/mL).
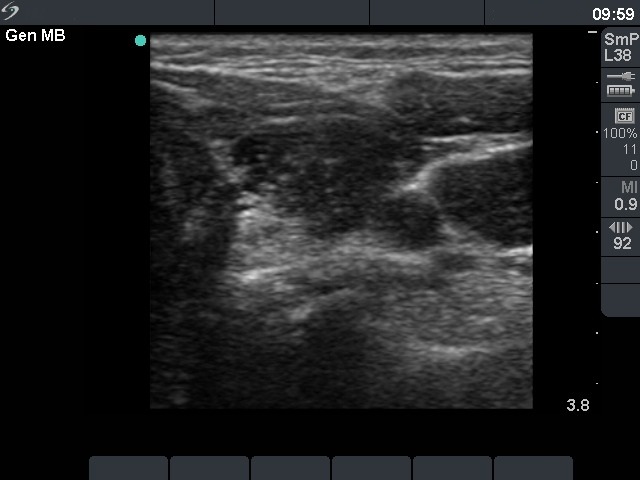
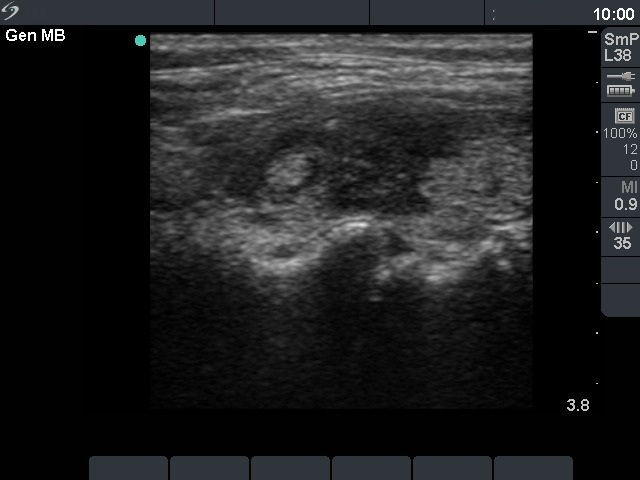
Ultrasonography. The thyroid was echonormal and presented several hypoechoic areas. The pattern in the right lobe was obviously focal form of lymphocytic thyroiditis.
A relatively large hypoechoic areas was found in the left lobe. The lesion had irregular borders. At first sight, this presentation of the left lobe could be interpreted as the central hypoechoic area-type form of lymphocytic thyroiditis. However, the hypoechoic lesion was not entirely surrounded with echonormal thyroid tissue. More importantly, the central hypoechoic areas-type form is almost always bilateral.
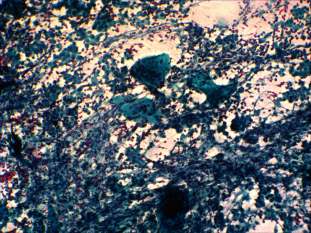
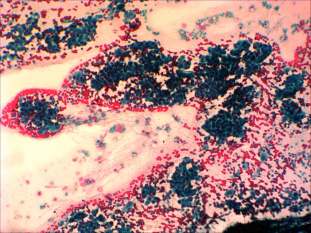
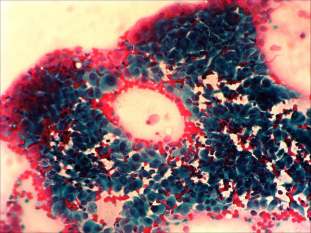
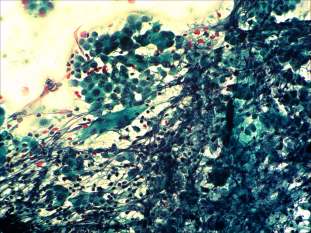
Cytological picture: There was no colloid in the background. Thyrocytes occurred in clusters and dissociated and exhibited oxyphilic metaplasia, prominent nucleoli, intranuclear inclusions and grooves. There were large number of heterogeneous lymphoid and several multinucleated giant cells on the smear.
Cytological diagnosis: papillary carcinoma. Hashimoto's thyroiditis.
Histopathology disclosed a T4 papillary carcinoma and Hashimoto's thyroiditis. The tumor invaded the wall of the trachea but did not brake into.
Comments.
-
We gained multiple smears from the tumor. There were signs of Hashimoto's thyroiditis in the presented smear, too, while this was the only finding on other smears.
-
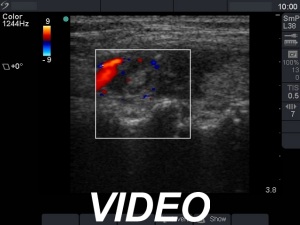
The sonographic pattern is remarkable. On the one hand, the tumor was identical to other more active foci of Hashimoto's thyroiditis. The only difference was the size of this lesion which was larger than other lesions observed in the thyroid. In the case of Hashimoto's thyroiditis neither the irregularity of border, nor the increased vascularization has any relevance. On the other hand, the tumor had microcalcifications and was significantly larger than other foci. The lesson to draw is the comparison of various lesions: if we detect a lesion which differs from others regarding the echogenicity, the size or the vascularization, it is advisable to perform FNA.
-
The distinction of central hypoechoic area-type form of LT from a large hypoechoic nodule is in part based on noticing whether the pattern is bilateral or unilateral. While the former is almost pathognomonic of LT, the latter excludes this special form of LT and significantly increases the probability of a true nodule.
.