
|
|
Lymphocytic thyroiditis - case 188
|
|



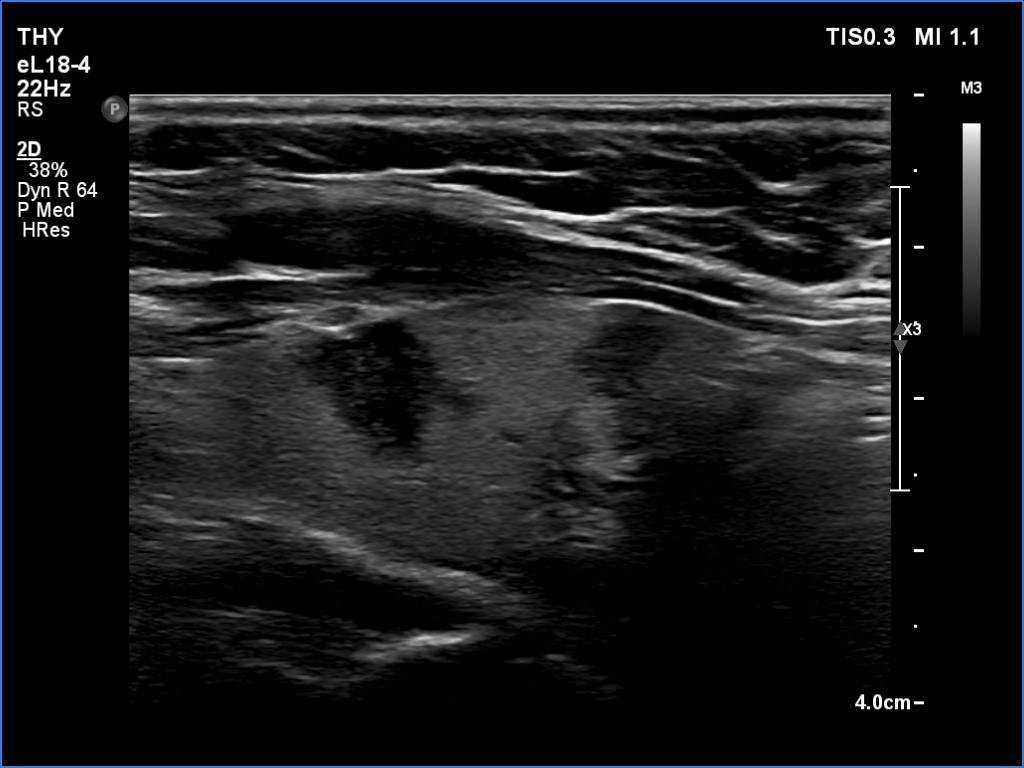
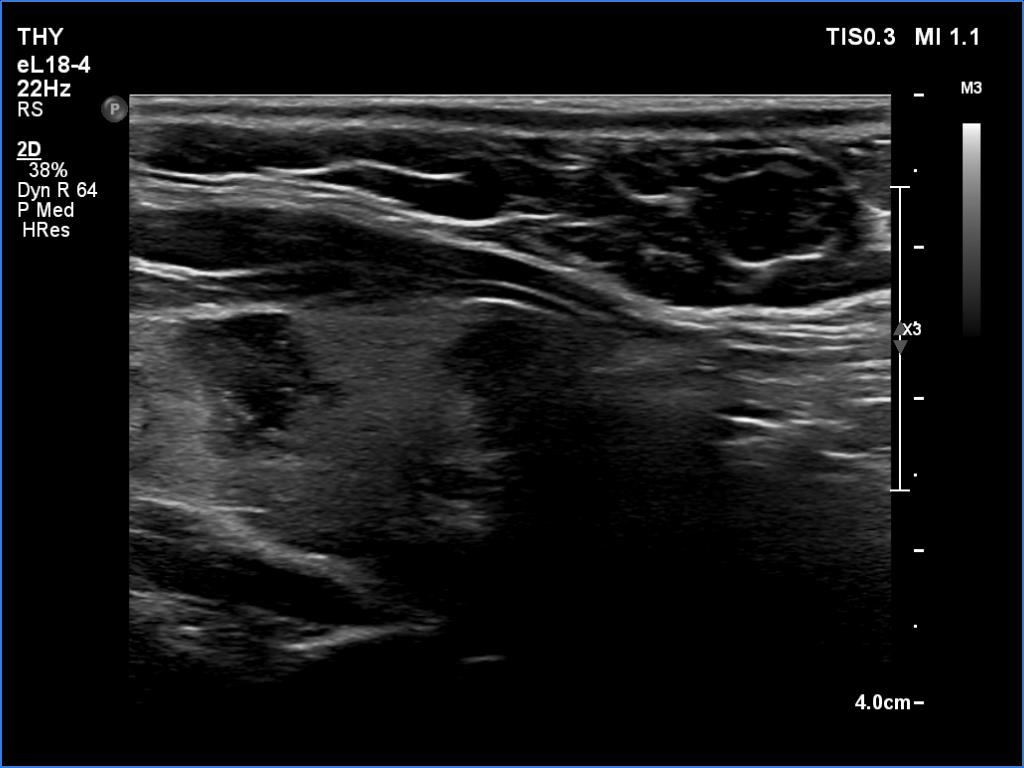

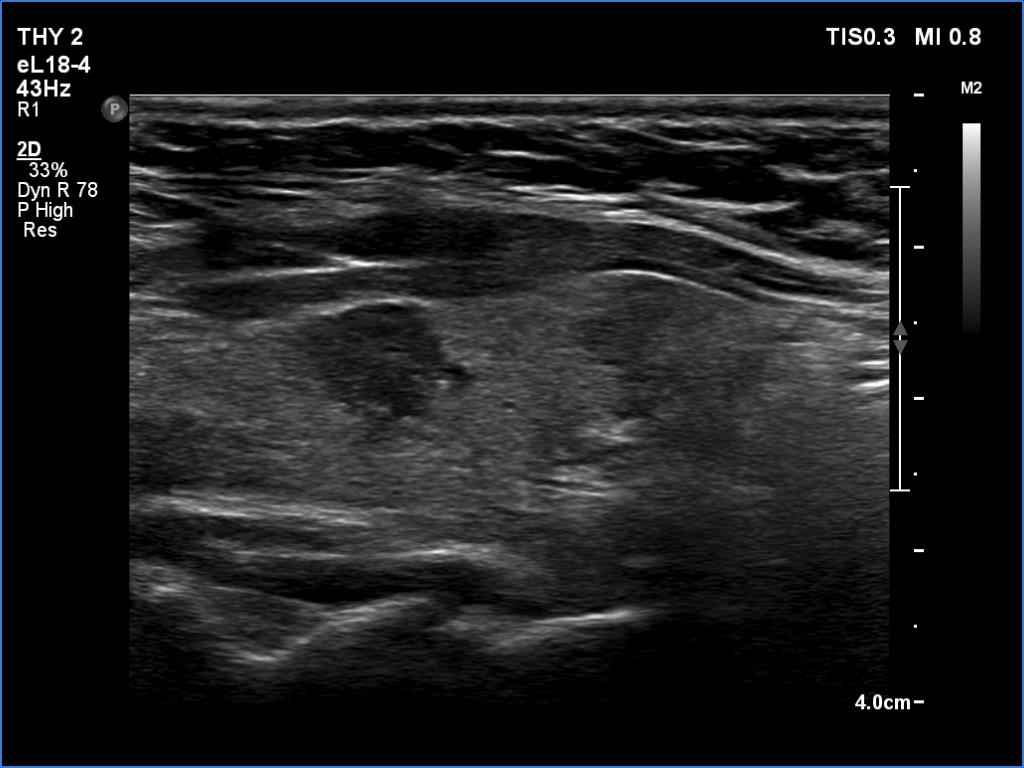


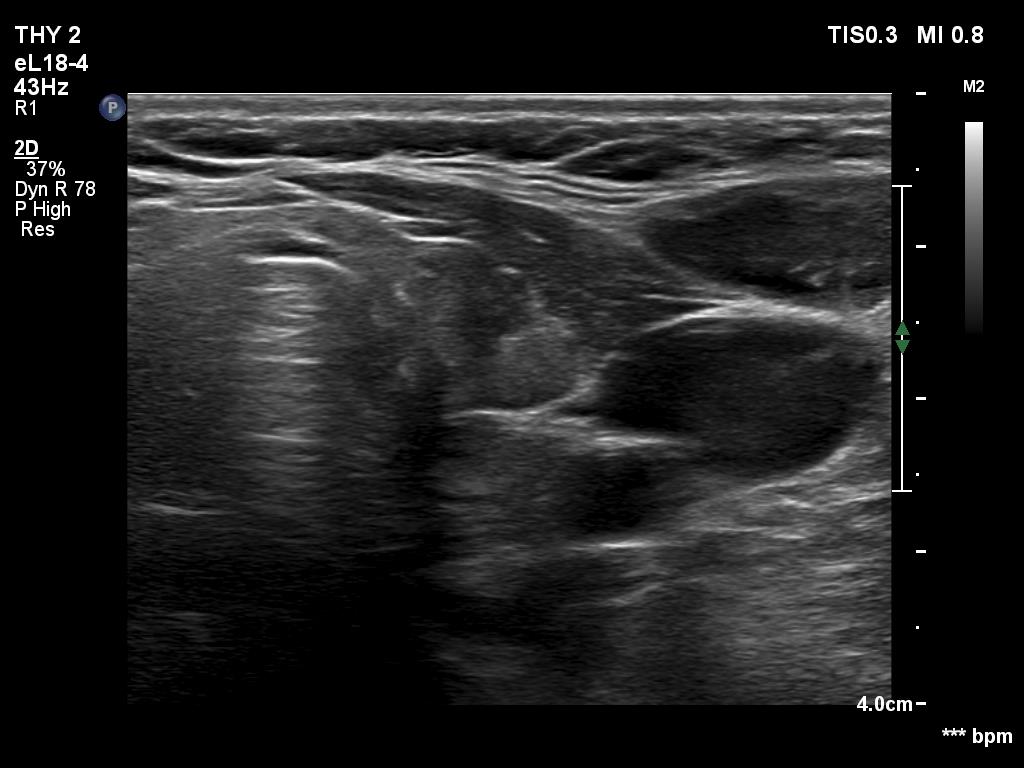

First examination (first and second rows of images):
Clinical data: A 37-year-old woman requested a screening. Recently, her mother was diagnosed with hypothyroidism and we suggested to screen the first-degree female relatives for autoimmune thyroid disease.
Palpation: no abnormality.
Laboratory tests: TSH 8.79 mIU/L, aTPO 808 U/mL.
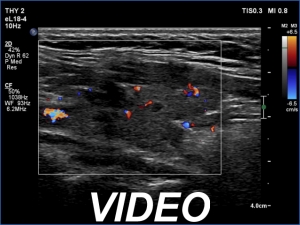
Ultrasonography. The thyroid was echonormal or minimally hypoechoic and had several discrete, more hypoechoic areas. Two of them in the left lobe were remarkable because of irregular borders and nonparallel orientation.
Cytology was performed from the larger lesion in the left lobe and resulted in Hashimoto's thyroiditis.
Daily 50 microgram levothyroxine was administered. We suggested repeat ultrasound and cytology in a year.
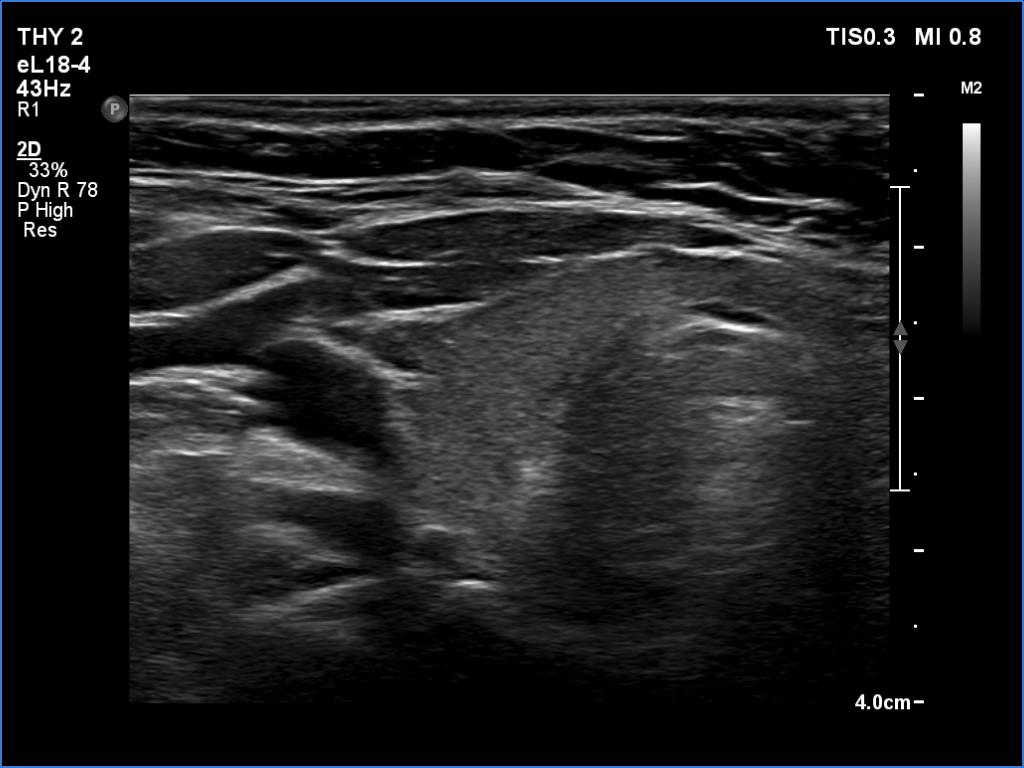
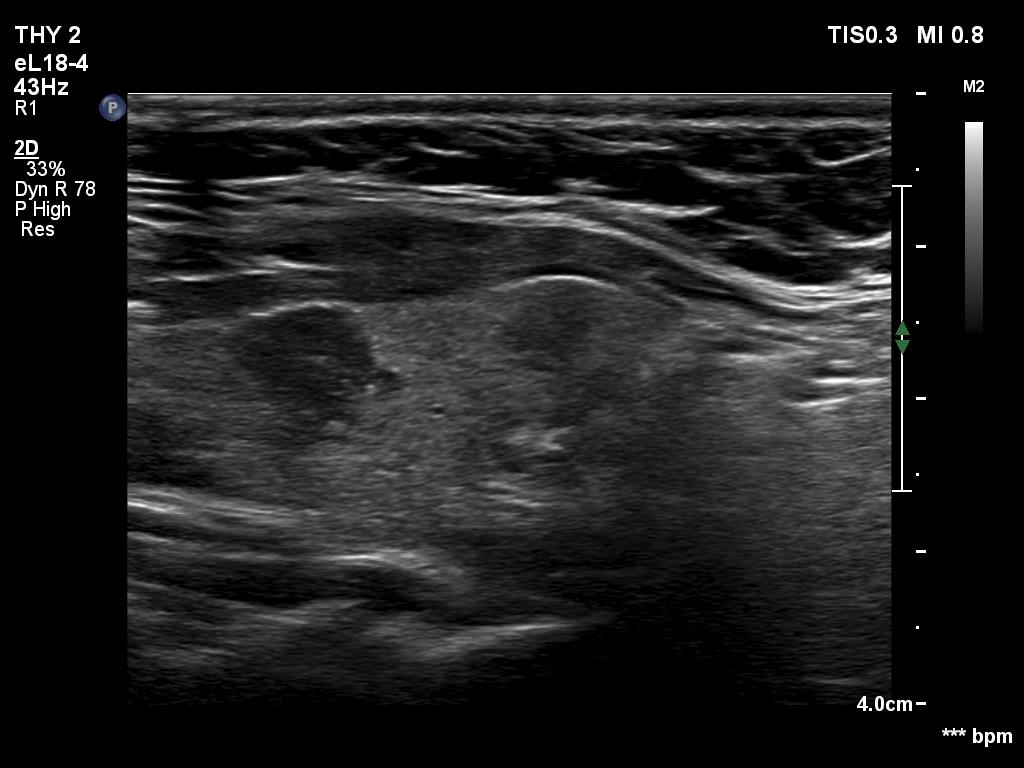
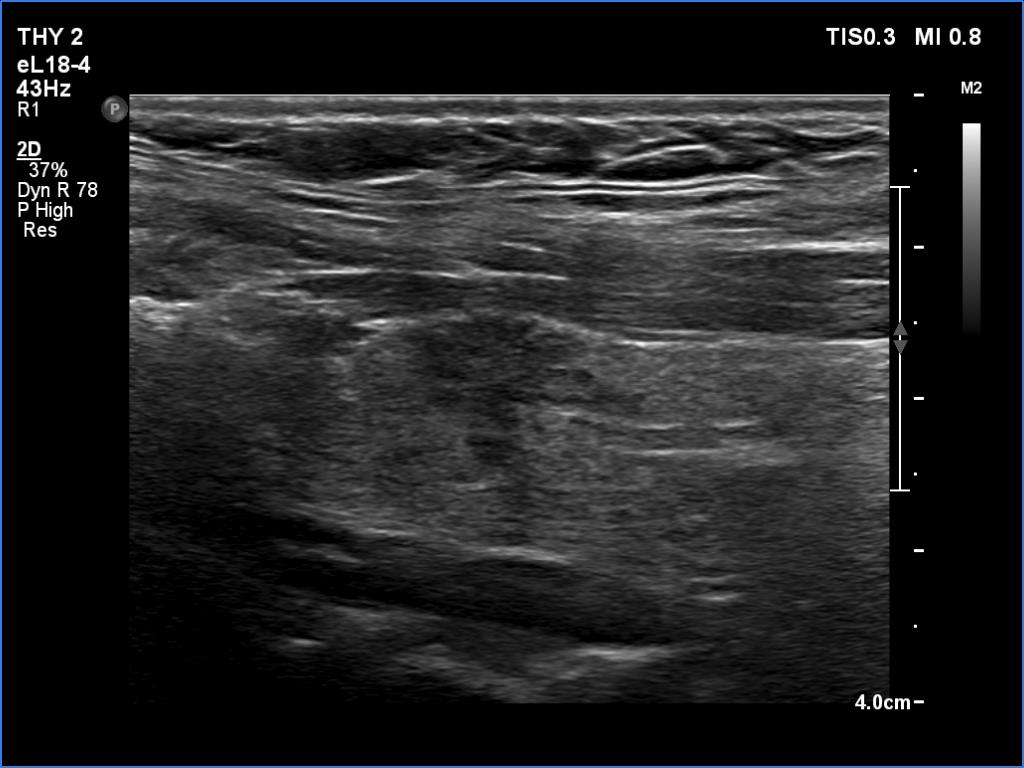
Second examination 2 years later (third rows of images):
Clinical data: The patient had no complaints.
Palpation: Both lobes were a bit firm on palpation. There was a not firm nodule in the right lobe.
Laboratory tests: TSH 2.05 mIU/L on daily 50 microgram levothyroxine.
Both the ultrasound and the cytological patterns remained unchanged.
Comments. The discrete lesion in the left lobe is highly suspicious, and even after two reassuring cytological findings, some suspicions remain. Two considerations. Firstly, the largest diameter of the lesion was 10 and 9 mm, first and second examination, respectively. All TIRADS are contradictory on the indication of cytology: according to their main tables, cytology is not justified, while all argue in the text that cytology may be considered in the case of a nodule with a suspicious sign no larger than 1 cm. Secondly, ultrasound follow-up is clearly advisable in such cases.