
|
|
Lymphocytic thyroiditis - case 897
|
|










First examination (first row of images):
Clinical data: A 22-year-old woman came to a follow-up examination. She has been diagnosed with euthyroid Hashimoto's thyroiditis for years. At that time, the aTPO was 380 U/mL. She had no complaints.
Palpation: no abnormality.
Laboratory tests: TSH 5.61 mIU/L.
Ultrasonography. The thyroid was echonormal or minimally hypoechoic and was decreased in size. There was no discrete lesion within.
Suggestion: Considering the age of the patient, replacement therapy with daily 50 microgram levothyroxine was started.
Second examination 6 years later (second row of images):
Clinical data: The TSH was regularly checked and remained within the normal range in the past 6 years on daily 50 microgram levothyroxine. Ultrasound was performed in every two years and the pattern was the same as at the first examination so far.
Palpation: no abnormality.
Laboratory tests: TSH 2.38 mIU/L on daily 50 microgram levothyroxine.
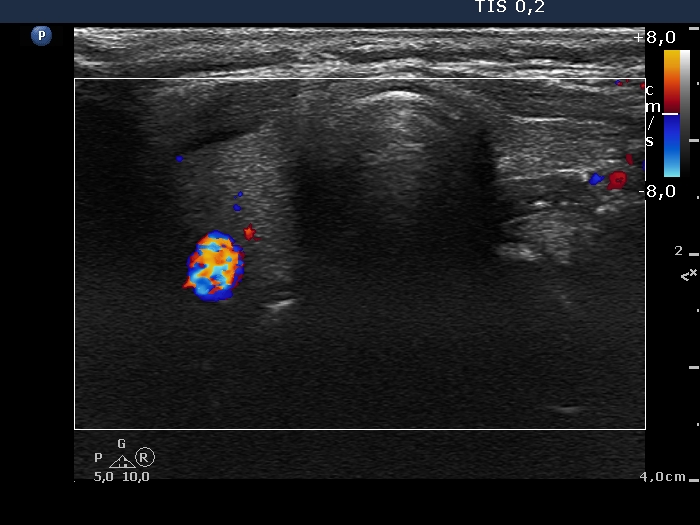
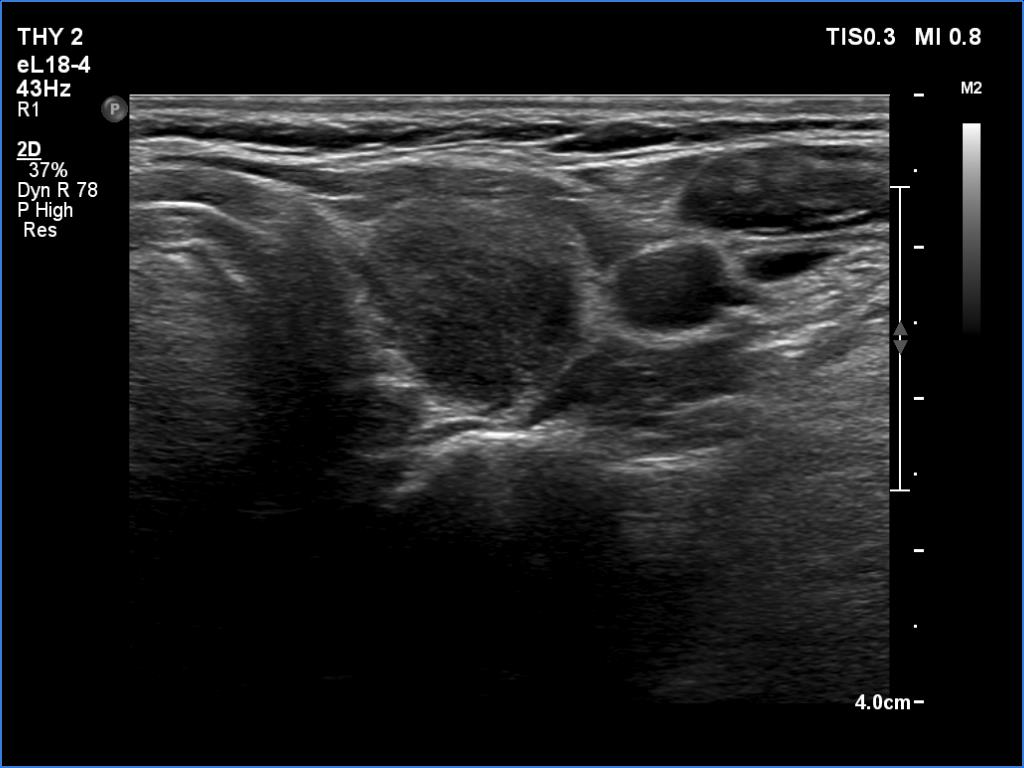
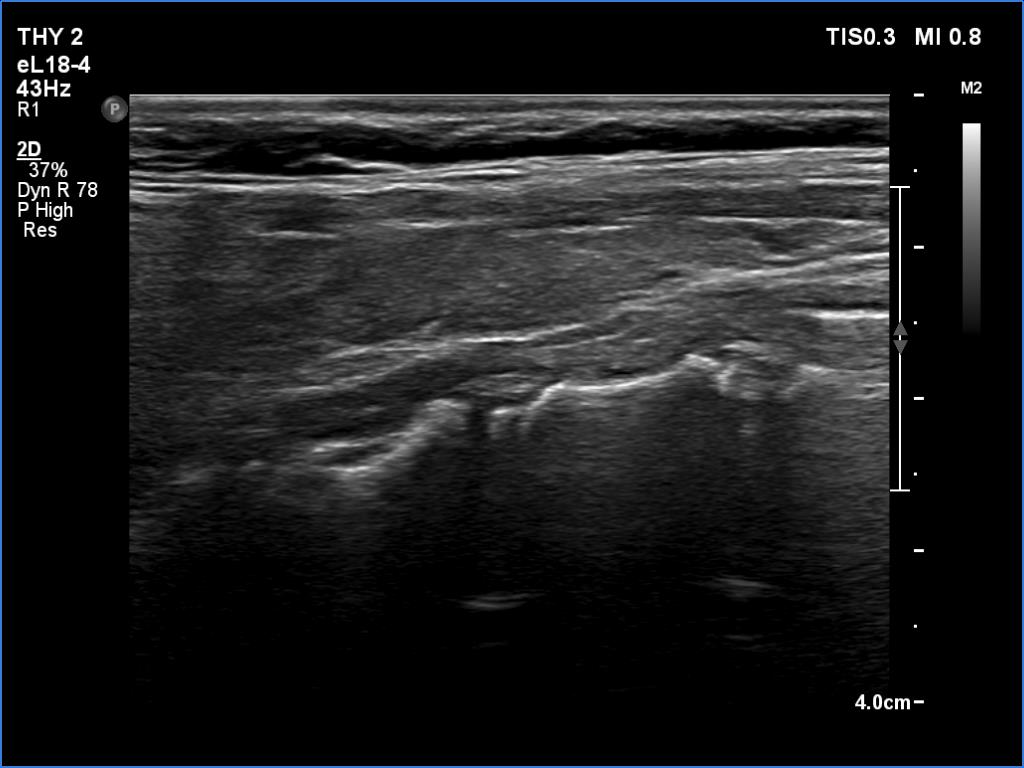
Ultrasonography. The right lobe was echonormal and had several minimally-moderately hypoechoic islets which presented relatively sharp borders. A moderately hypoechoic lesion has appeared in the left lobe. The lesion had blurred borders and was avascular.
Additional tests: aTPO 7 U/mL, CRP 0.8 mg/L.
Aspiration cytology resulted in Hashimoto's thyroiditis.
Suggestion: daily 50 microgram levothyroxine. Repeat ultrasound in 3 to 6 months.
Third examination 6 months after the previous visit (third row of images):
Clinical data: The patient had no complaints.
Palpation: no abnormality.
Laboratory tests: TSH 2.97 mIU/L, aTPO 28 U/mL on daily 50 microgram levothyroxine.
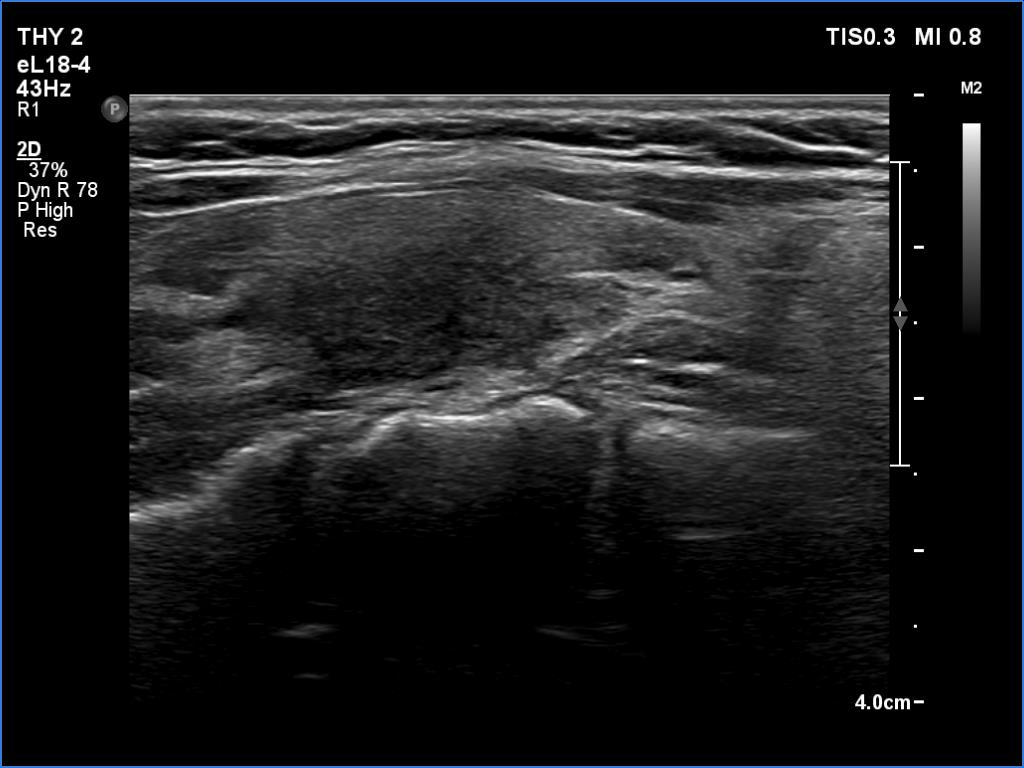
Ultrasonography. The pattern remained unchanged except for the disappearance of the large, ill-defined lesion in the left lobe.
Suggestion: daily 50 microgram levothyroxine, TSH in a year.
Comments.
-
The change in the echo pattern is not a rare phenomenon in lymphocytic thyroiditis. However, it happens during years or decades. The exceptions are post partum thyroiditis and the so-called Hashitoxicosis. In the latter event, upper airways infection activates the underlying thyroiditis and leads to a temporary increase of thyroid hormone levels. The change in ultrasound pattern cannot be unequivocally explained with the former circumstances. The patient was not pregnant, and the thyroid hormones were stable. Despite the normal CRP level, a subacute, de Quervain's thyroiditis should be also considered.
-
It is worth noting the difference between the ultrasound and aTPO level. At first time, the former did not disclose autoimmune process while the aTPO level did, while at the follow-up visit the situation was completely the opposite.