
|
|
Case 1358
|
|





Clinical data: A 47-year-old woman requested a second opinion. She has been operated for a T3, conventional-type of papillary cancer for 4 years. Total thyroidectomy and radioiodine therapy were performed and she was regularly checked for thyroglobulin which was always undetectable. Recently, two lesions suspicious of recurrence were described on ultrasound.
Palpation: no abnormality.
Laboratory tests: TSH 0.07 mIU/L, FT4 23.6 pM/L, thyroglobulin below 0.2 ng/mL, anti-hTg below 20 U/mL on daily 125 microgram levothyroxine.
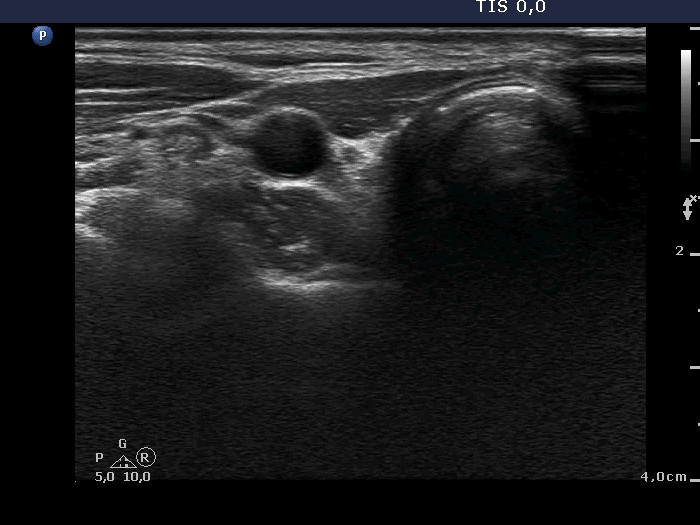
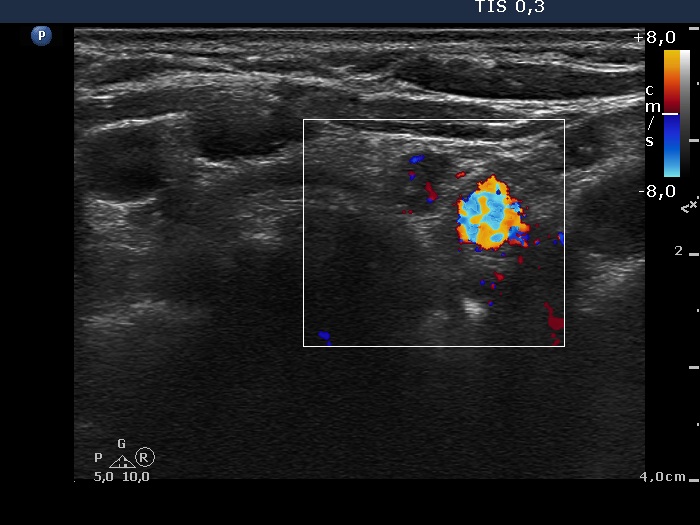
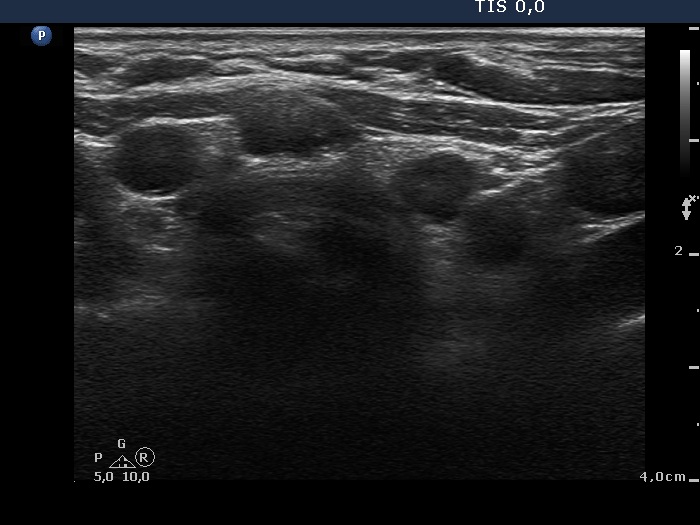
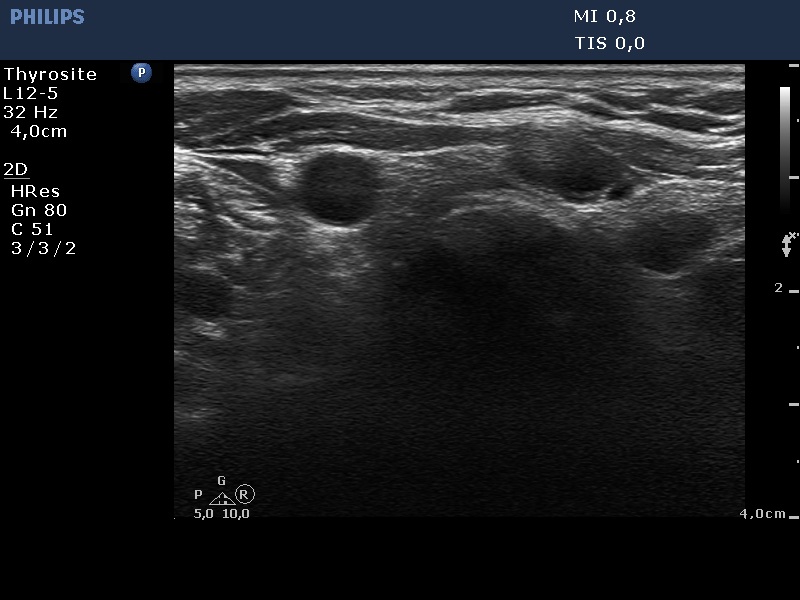
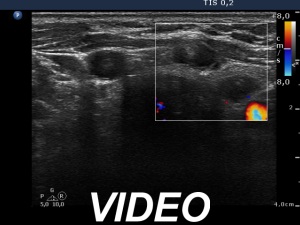
Ultrasound. Connective tissue replaced the thyroid parenchyma in both thyroid beds. There were tiny hypoechoic areas in the right thyroid bed. Two larger hypoechoic lesions were found, one in the isthmus and the other in the left thyroid bed. The latter presented vascularity.
Aspiration cytology from the larger lesions was non diagnostic. Thyroglobulin could not be detected in the wash-out.
Suggestion: continuation with the follow-up.
Comment. The presentations of the hypoechoic lesion in all three sites were the same, they differed only in their size. Naturally, the two larger in the isthmus and in the left thyroid bed could cause and did cause concern. Especially that in the left lobe due to its intralesional vascularity. The larger lesions can correspond to small muscle fibers, remnant of the regenerative provess after the surgery but even damaged, non-viable thyroid tissue. Taking the thyroglobulin level into account, the risk of thyroid cancer is minimal but not zero.