
|
|
Case 856
|
|







First examination (first row of images)
Clinical data: A 42-year-old woman requested a second opinion. She has been operated on for 3 months. A left lobectomy was performed, and histopathology disclosed a solitary, T2 papillary cancer. No further therapy was suggested.
Palpation: No abnormality.
Hormonal investigation indicated euthyroidism with TSH-level 2.56 mIU/L.
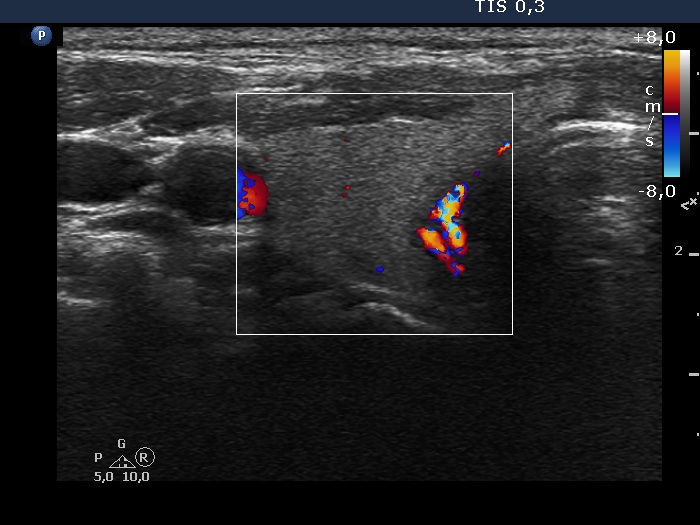
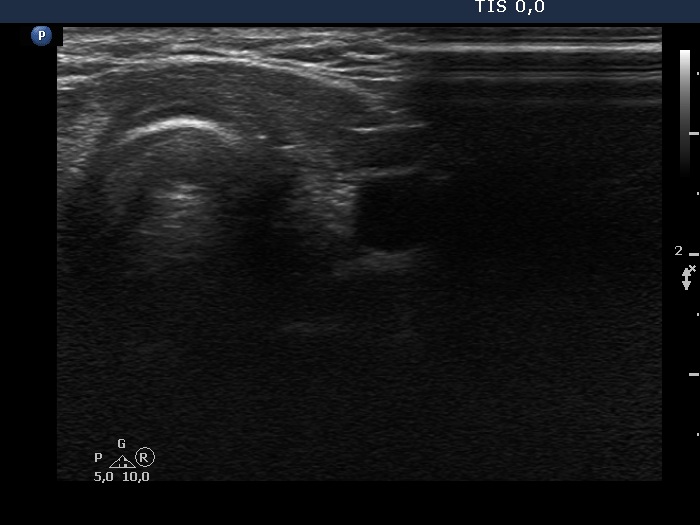
Ultrasonography. The right lobe was echonormal and intact. A hypoechoic, regenerative tissue was found in the isthmus and in the left thyroid bed. A small, deeply hypoechoic lesion was found in the middle of the left thyroid bed with the dimensions of 3x3x4 mm, width, depth and length, respectively.
Suggestion. I agreed with the suggestion of the surgeon. Yearly TSH and ultrasound was advised.
Second examination a year later (second row of images)
Clinical data: The patient had no complaints except for COVID-19 infection 3 months before the present visit.
Palpation: unchanged.
Hormonal investigation: TSH 3.10 mIU/L.
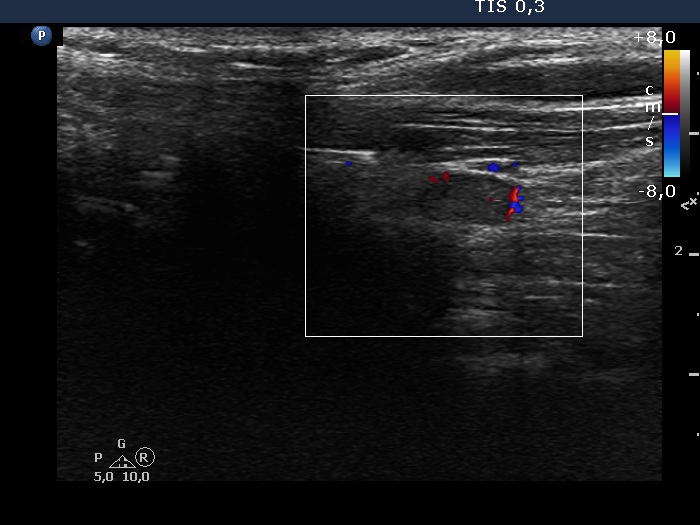
Ultrasonography revealed that the discrete hypoechoic lesion in the left lobe had increased in size, the dimensions were 4x4x5 mm, width, depth and length, respectively. There was a lymph node lateral to the left lobe. The node presented a heterogeneous pattern and lacked a regular hilum.Suggestion: repeat ultrasound in 3 to 6 months.
Comments.
-
The small hypoechoic lesion within the left thyroid corresponds to a remnant. It seems to be realistic that this is thyroid tissue, but we have no particular reason to assume it would be a malignant lesion.
-
However, the lymph node is suspicious, especially due to its heterogeneity.