
|
|
Case conp 041
|
|















First examination (1st to third rows of images):
Clinical data: A 14-year-old boy was referred for evaluation of a nodule discovered by himself.
Palpation: a hard, not freely moveable nodule in the isthmic part of the left lobe.
Hormonal examination: indicated euthyroidism with TSH 2.09 mIU/L.
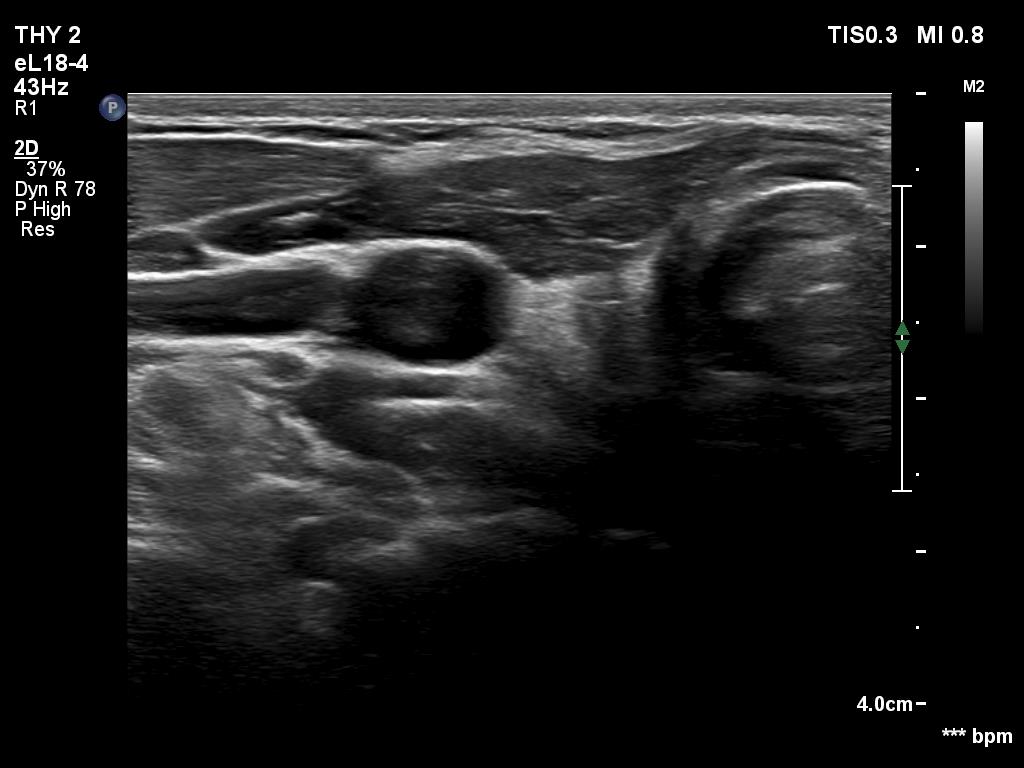
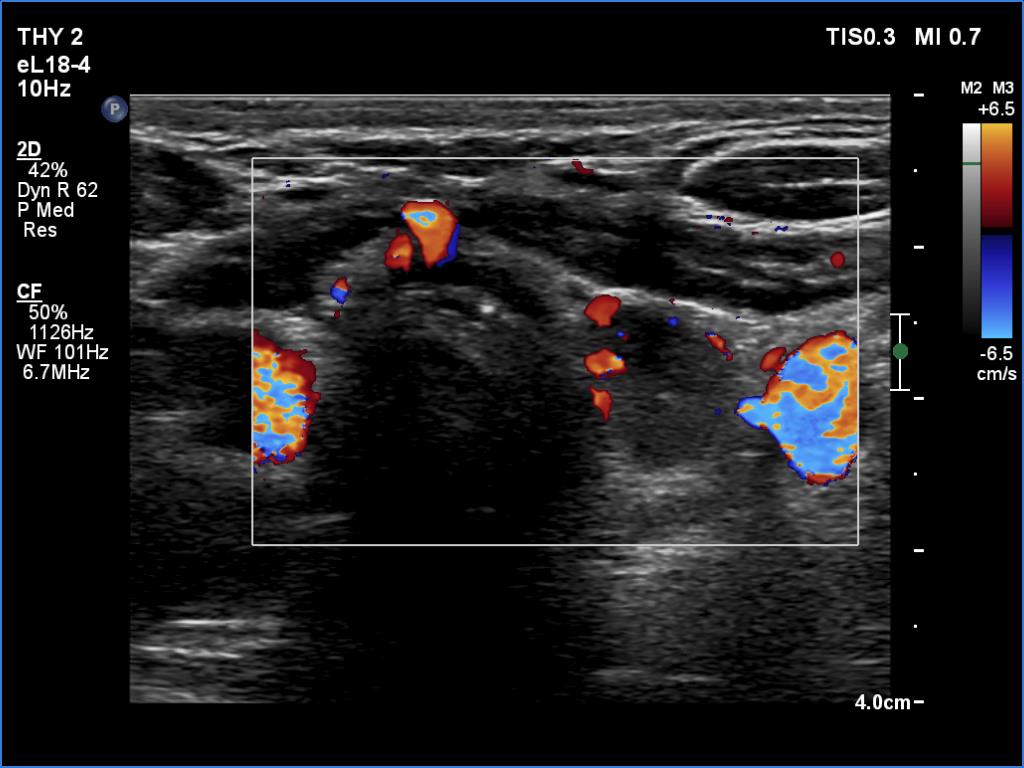
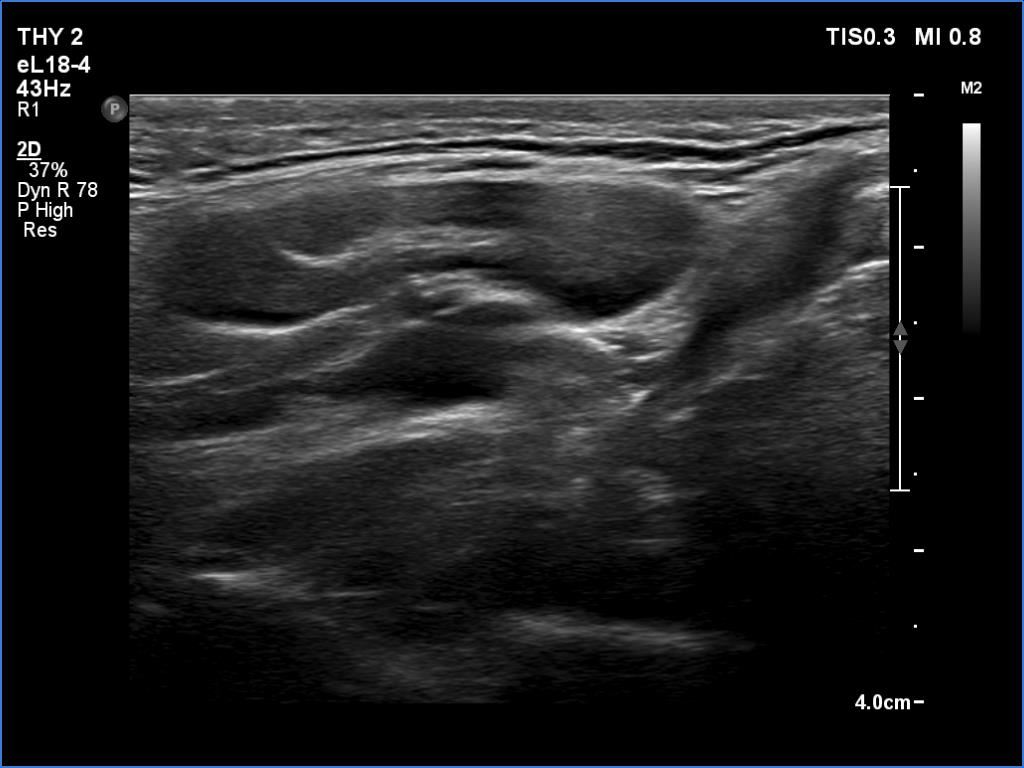
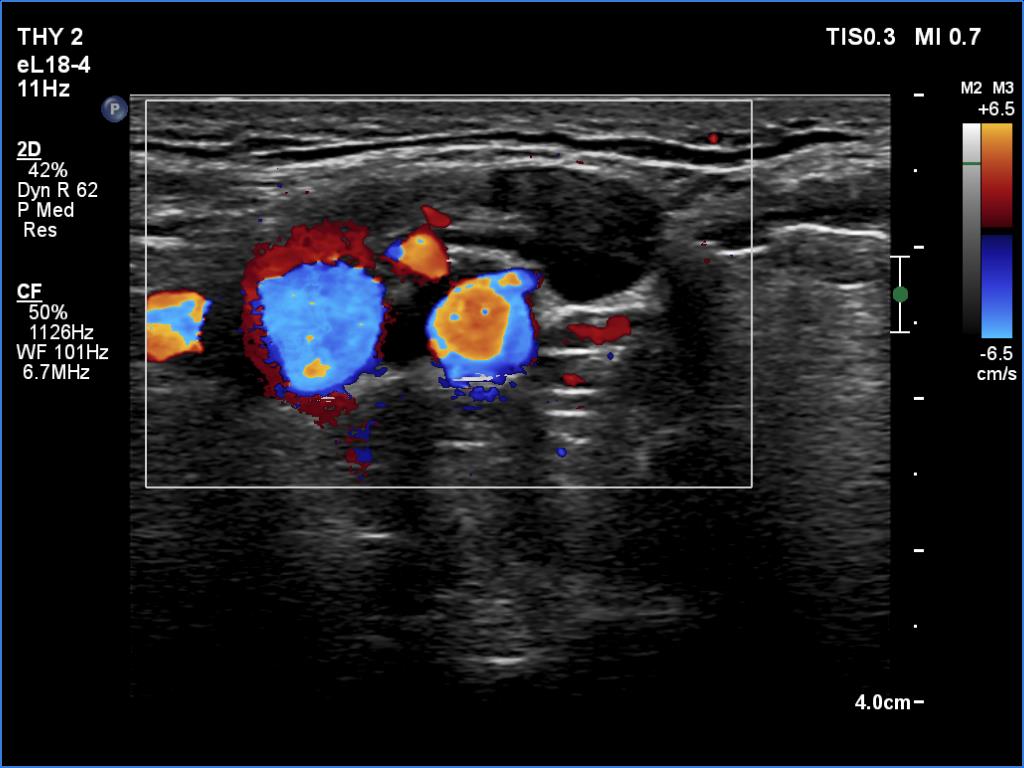
Ultrasonography revealed a hypoechogenic nodule in the ventromedial part of the left lobe. The nodule had irregular borders, contained microcalcifications and displayed perinodular and irregular intranodular blood flow.
Cytology: follicular tumor.
Based on the ultrasound and cytological pattern combined, the probability of cancer was greater than the average.
Histopathology disclosed an embryonal-type follicular adenoma in the left lobe. Almost the entire lobe was consisted of the adenoma. There were within the nodule large fields of lymphocytic infiltration. In the middle portion of the nodule a papillary carcinoma was found with a maximal diameter of 15 mm with metastasis to 3 of the removed 9 lymph nodes in the left side of the neck.
Comments.
It is evident that the cytological material was gained not from the papillary carcinoma but from the adenoma.
It is hard to decide which portion of the lesion corresponded to the carcinoma
Follow-up examination 8 years later (4th and 5th rows of images):
Clinical data: The patient was referred for evaluation of a continuously increasing thyroglobulin level which resulted in 2.86 ng/mL, 5.74 ng/mL and 20.1 ng/mL, at the 2-yr, 5-yr and 7-yr follow up. Cytology of enlarged lymph nodes, multiple CT-scans and PET-CTs failed to reveal recurrence.
Palpation: There were two palpable, firm but freely moveable masses in the right and left submandibular area.
Hormonal examination: indicated euthyroidism with TSH 2.95 mIU/l on daily 125 microgram levothyroxine. Thyroglobulin was 15.4 ng/mL, anti-hTg was below 20 U/mL.
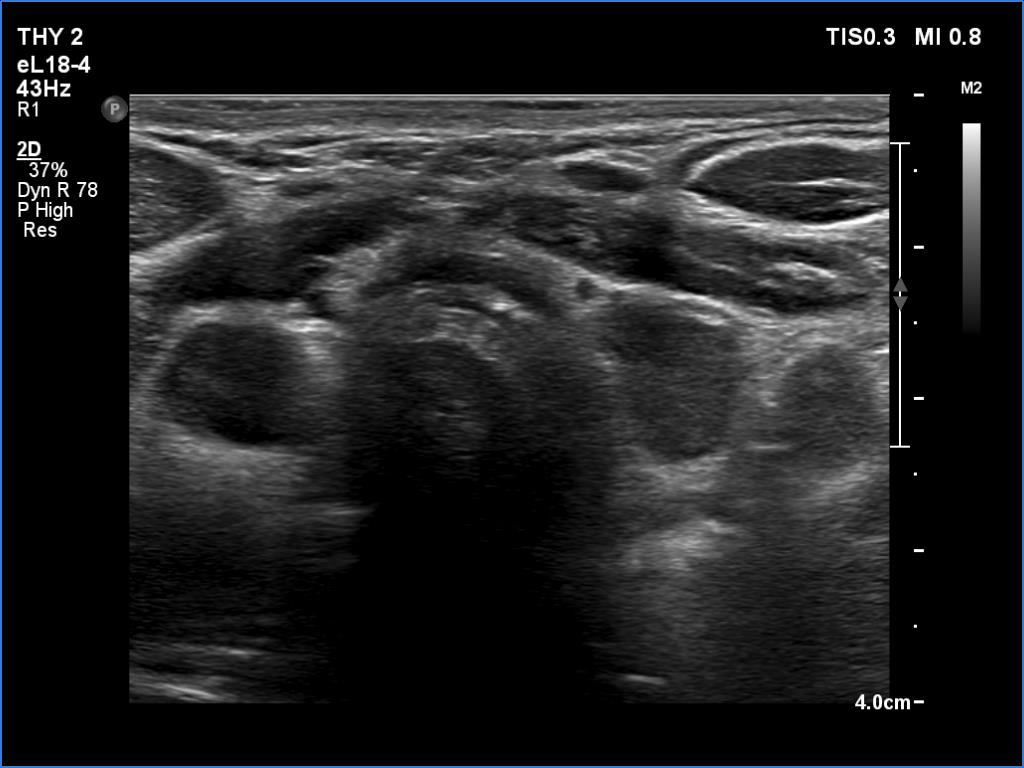
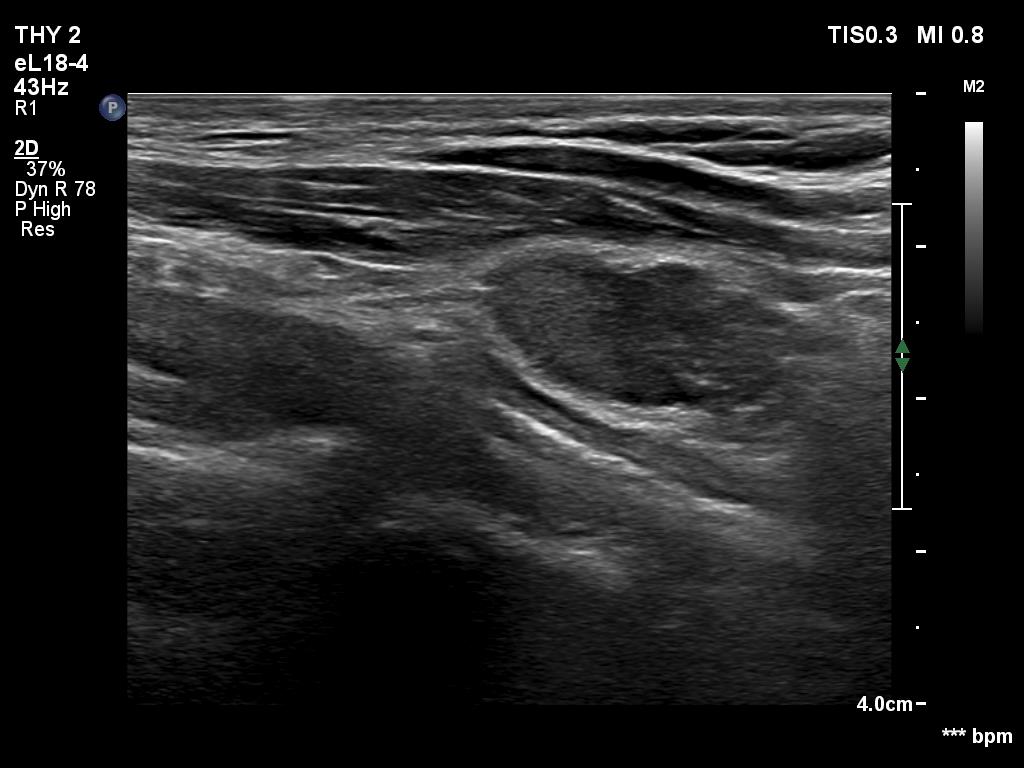
Ultrasonography revealed hypoechoic discrete lesions in both thyroid lobes. The lesions presented microcalcifications. Corresponding to the palpable mass in the right submandibular region, a reactive-type regular lymph node was found. There was an enlarged lymph node in the left submandibular region. The node had a regular hilum but displayed a heterogeneous pattern.
Cytology was performed from both lymph nodes and from the lesion in the left thyroid bed. FNA resulted in non-diagnostic report from the lesion in the left thyroid bed while cytology of the submandibular lymph nodes showed patterns of a benign, reactive-type lymph node.
Wash-out thyroglobulin levels were 0, 81.1 and 104.9 ng/mL, right submandibular lymph node, left thyroid bed lesion and left submandibular lymph node, respectively.
Histopathology in progress.
Comment. Until the final histological examination is completed, I would like to draw attention to two things. One is the heterogeneity of the left lymph node and the other is the size and structure of the lesions in the thyroid beds - these features are suspicious of thyroid cancer.
.