
|
|
Study on 100 consecutive patients with thyroid nodule - case 048
|
|







Clinical presentation: A 67-year-old woman was referred for aspiration cytology of a recurrent nodule. A left subtotal lobectomy was performed 19 years ago, histopathology resulted in benign lesion not otherwise specified. She noticed a rapidly growing mass in the right lobe which caused neck discomfort.
Palpation: a firm nodule in the right lobe.
Functional state: euthyroidism (TSH 3.08 mIU/L).
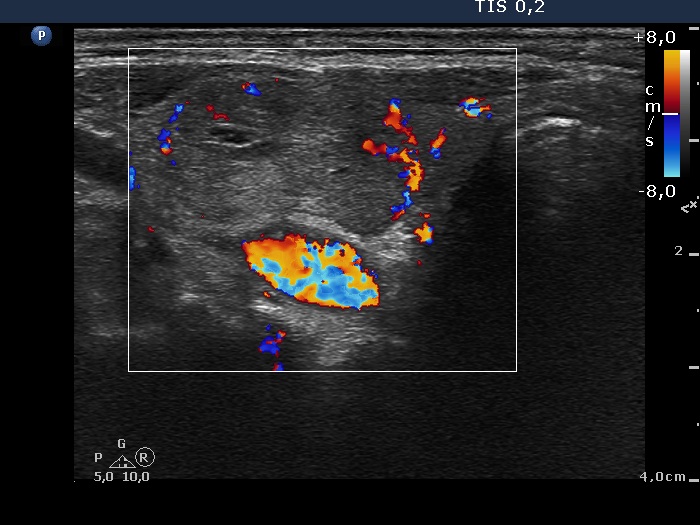
Ultrasonography. The thyroid was echonormal. A large nodular area occupied great part of the right lobe. This area was composed of discrete lesions with different echogenicities. The nodular are presented signs of perinodular blood flow. There were small discrete lesions in the left lobe.
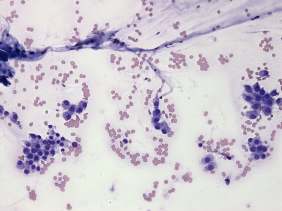
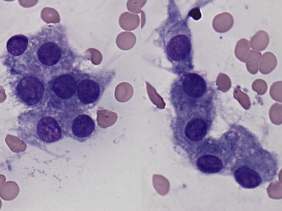
Cytology was performed from the nodule in the right lobe.
We gave a common ultrasound-cytological diagnosis of follicular tumor.
Histopathology revealed benign hyperplastic nodules.
Comments.
-
It is worth analyzing the ultrasound presentation. At first sight, a follicular tumor seems very likely: a large solitary nodule with halo sign occupies great proportion of a lobe. However, a more thorough analysis reveals that this large nodular area is composed of discrete lesions; although this feature does not exclude a follicular tumor, it significantly reduces this possibility.
-
The cytological pattern is also remarkable. Although the lack of colloid and the presence of microfollicles raise the possibility of a follicular tumor, the whole pattern is more likely correspond to a non-tumorous lesion.
-
I think that my diagnosis has failed: taking the ultrasound and cytological properties into account, the correct diagnosis would be benign lesion.