
|
|
100 consecutive cases of papillary cancer - case 096
|
|








Clinical data: A 54-year-old woman was referred for evaluation of a nodular goiter discovered on screening.
Palpation: Both lobes were firm but no nodule could be palpated.
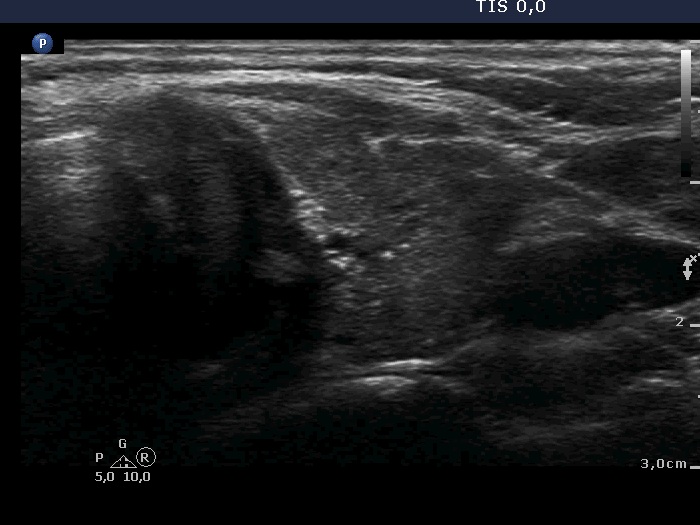
Ultrasonography. The thyroid was minimally hypoechoic and had more hypoechoic areas corresponding to the underlying thyroiditis. There was a nodule in the dorsal part of the left lobe. The nodule was a bit brighter compared to the extranodular tissue but darker compared to a healthy thyroid. Beside macrocalcification, the nodule contained numerous microcalcifications. The latter occurred even outside the tumor. The borders of the nodule were difficult to judge. The lesion presented a combined perinodular and intranodular vascularity.
Cytology was performed form the nodule. We gained irregular groups of oxyphilic cells mixed with lymphoid elements from the single attempt of aspiration. The patient did not permit more punctures.
Combined cytological-ultrasound diagnosis was suspicion of papillary cancer and Hashimoto's thyroiditis. Based on the suspicion of invasive spread, total thyroidectomy was indicated.
Laboratory tests: TSH 2.52 mIU/L, aTPO exceeded 1051 U/mL.
Histopathology disclosed a multifocal T4 papillary cancer in the left lobe. The tumor invaded the wall of the trachea but did not break into. Hashimoto's thyroiditis was found in the extranodular tissue.
Comments.
-
It is a rare situation that we cannot convince a patient to undergo on FNA. It is often necessary to resort to unique solutions. In this case, we offered the patient a settlement that we take only one sample instead of the recommended two or three samplings. In this patient, it was not a difficult choice even when faced with the cytological material because the ultrasound pattern itself was more than suspicious. The video is clearly superior to the recorded and presented images.
-
The extrathyroidal spread toward medial direction, i.e., the invasion of the trachea, is almost always impossible to judge because the cartilaginous wall of the traches hinders the evaluation of ultrasound signs of extrathyroidal extension.
-
Depending on the 'normal' reference tissue, the lesion can be regarded as iso/hyperechoic or minimally/moderately hypoechoic, the reference tissue is the non-nodular part of the actual patient or a healthy thyroid, respectively.
-
This is an example of invasive spread which is characterized by isolated microcalcifications relatively far from the primary tumor focus.