
|
|
The echogenicity of the nodule - case 365
|
|


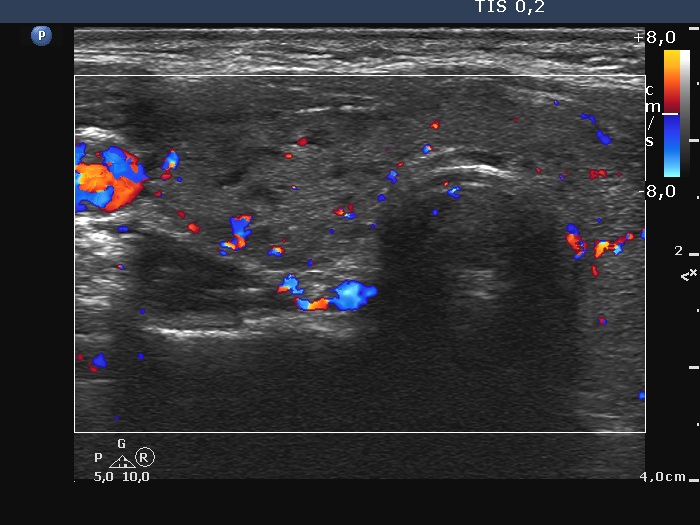

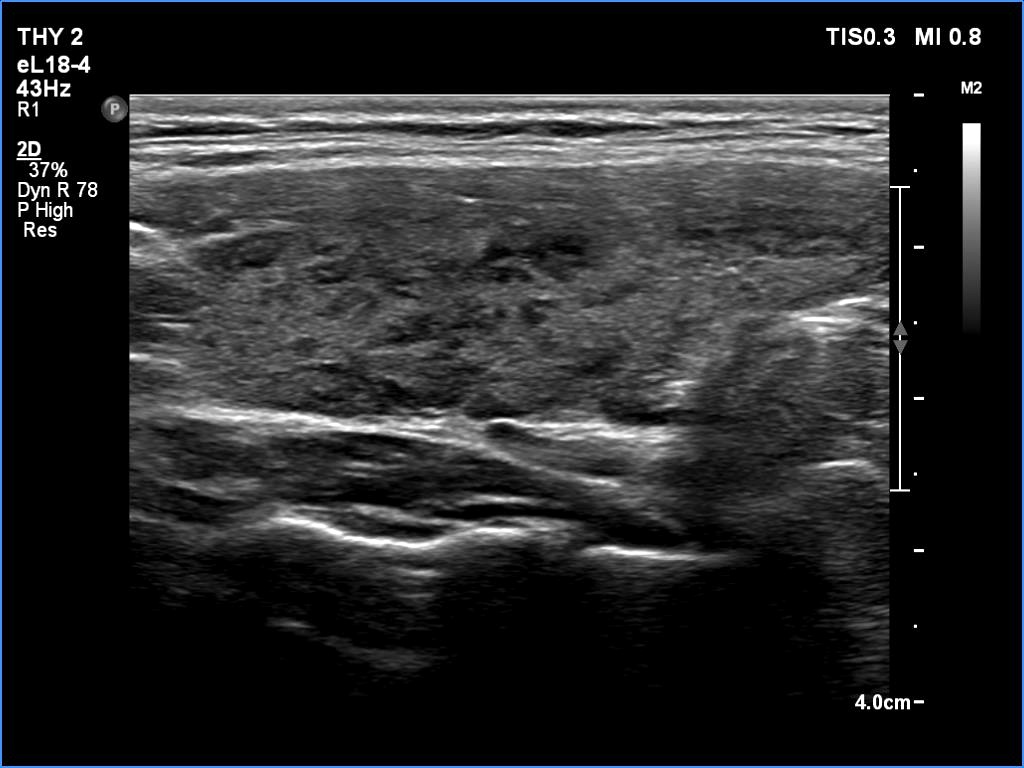



First examination (first row of images)
Clinical presentation: A 20-yr-old woman was referred for ultrasound examination. An elevated aTPO level was detected on evaluation of dysmenorrhea.
Palpation: Both lobes were firm. The left lobe was suspicious having a nodule.
Laboratory tests: TSH 2.08 mIU/L, FT4 13.2 pM/L, aTPO > 1300 U/mL.
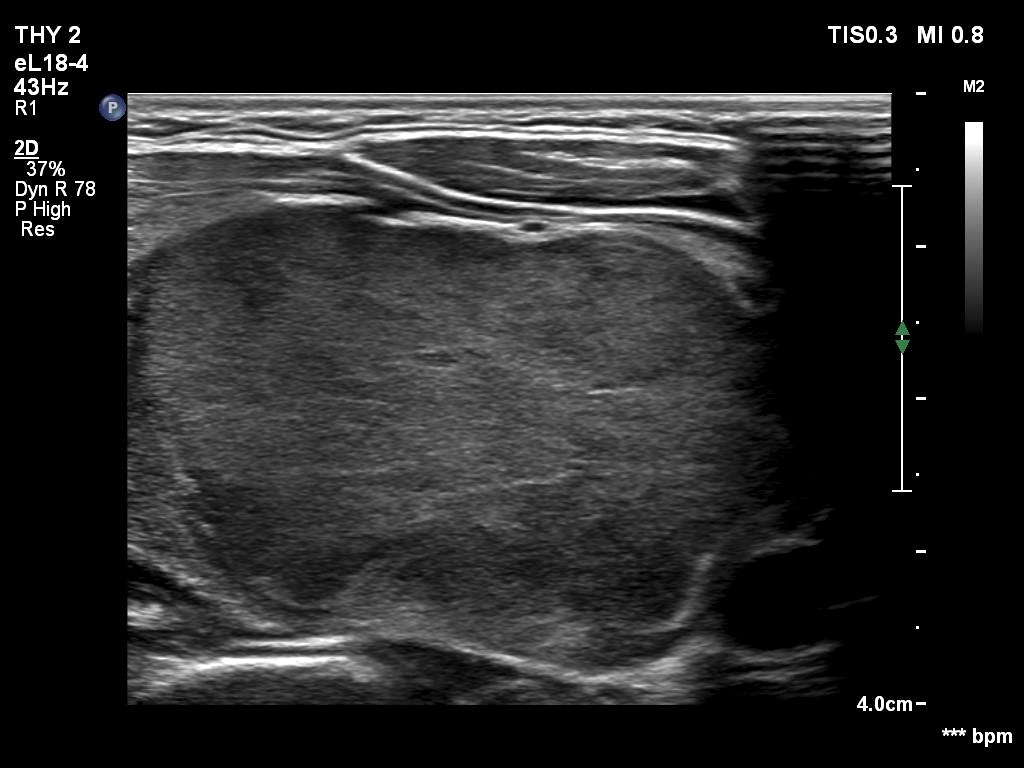
The dimensions of the nodule in the left lobe were 18x17x22 mm, width, depth, length, respectively, the volume of the lesion was 3.5 mL.
The patient did not consent to aspiration cytology.
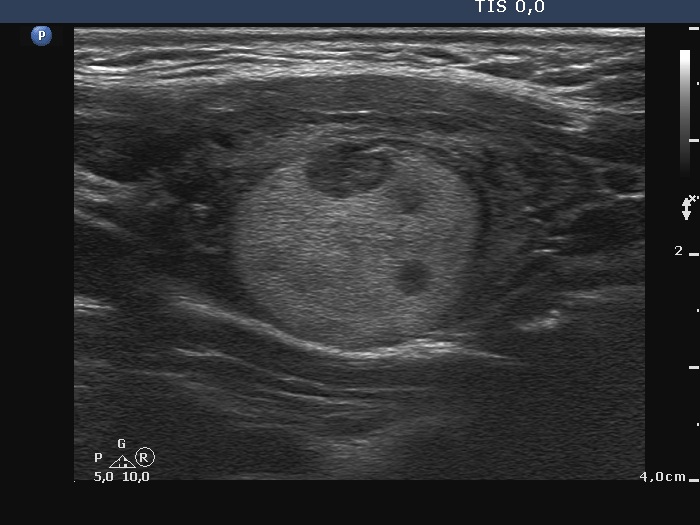
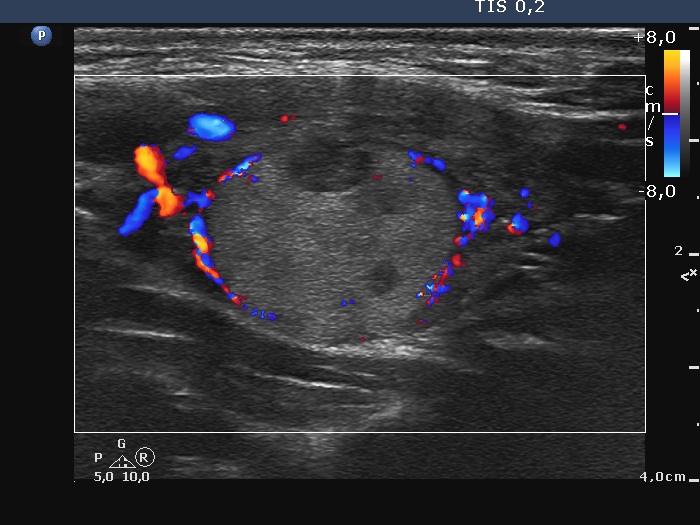
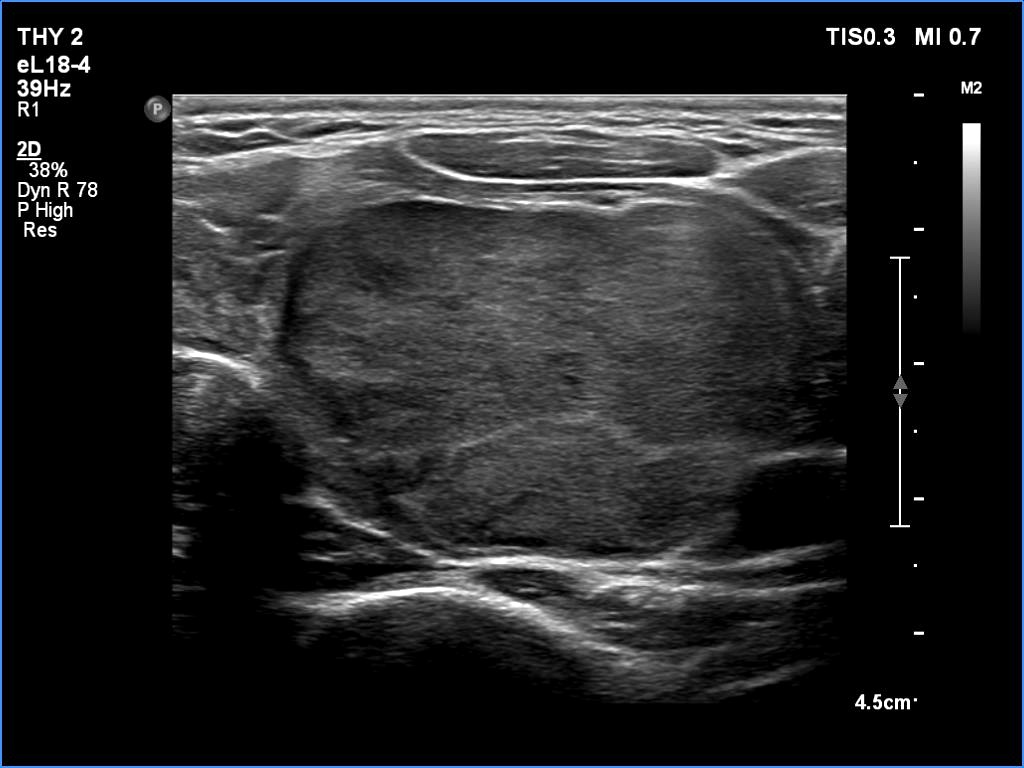
Second examination - five years later (second row of images)
Clinical presentation: The patient came to follow-up because she noticed a slow increase in the size of the left lobe.
Palpation: a firm nodule in the left lobe.
Laboratory tests: TSH 0.98 mIU/L.
The dimensions of the nodule in the left lobe were 40x25x43 mm, width, depth, length, respectively, the volume of the lesion was 22.5 mL.
Aspiration cytology resulted in follicular tumor. Surgery was advised.
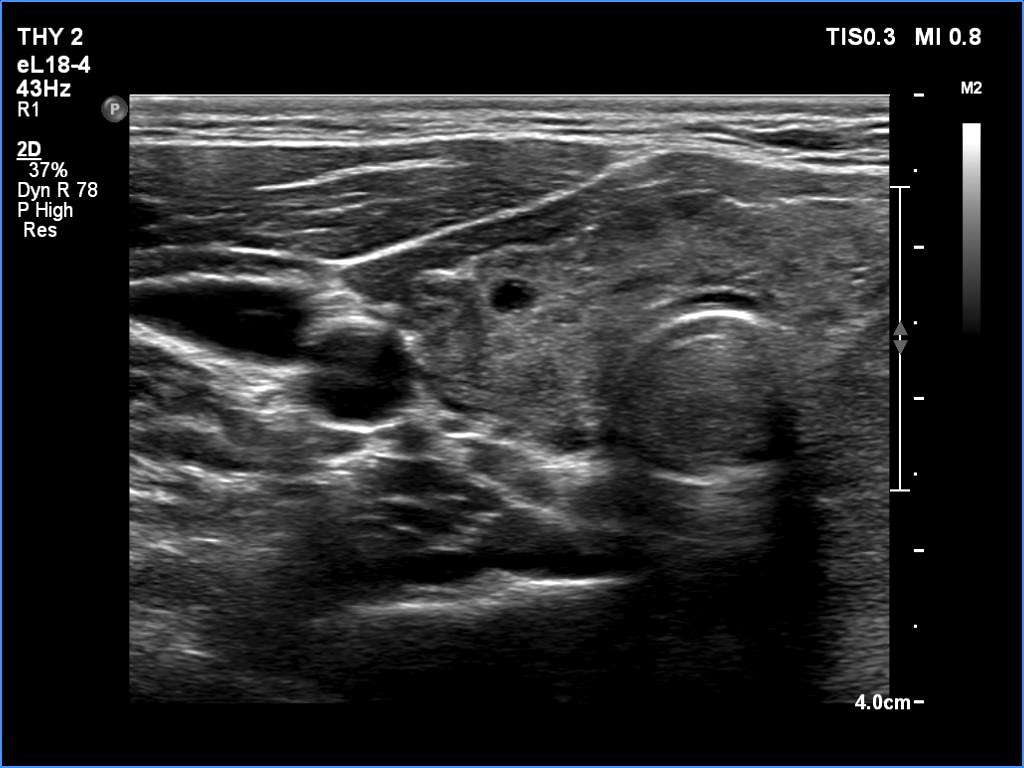
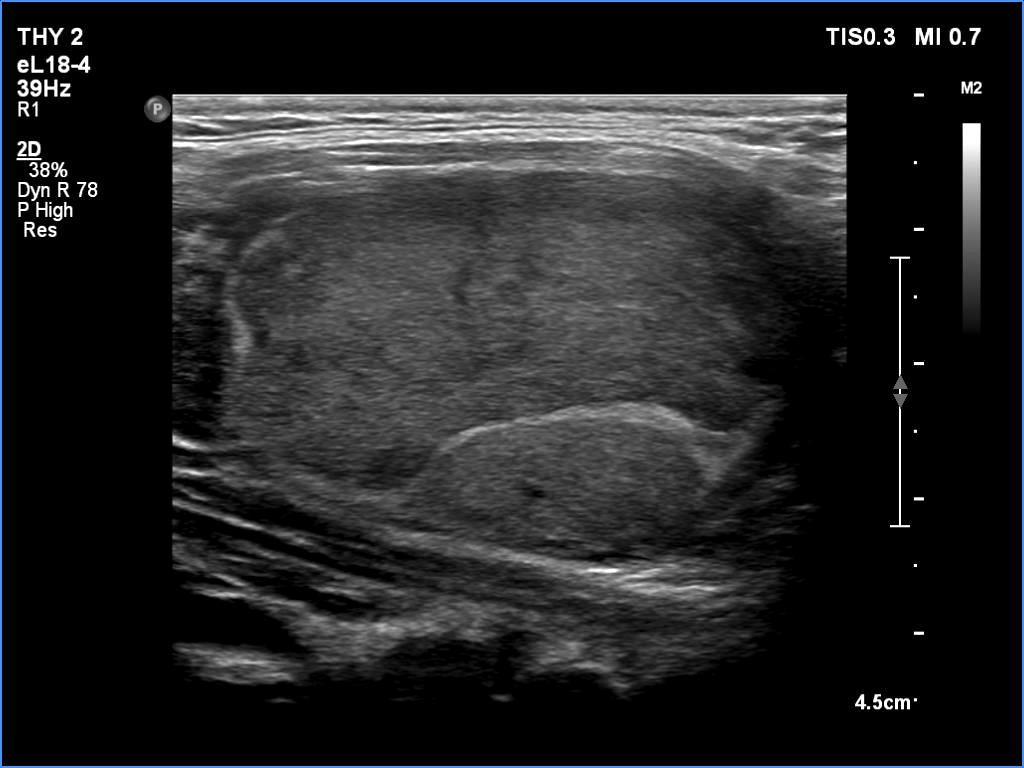
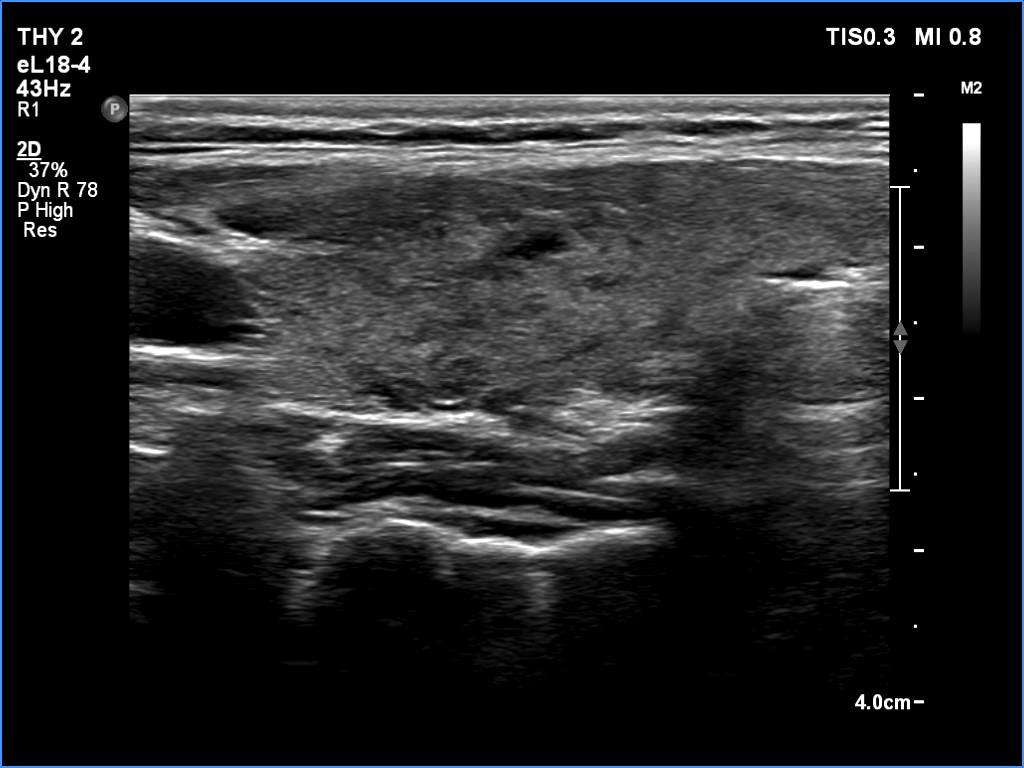
Third examination - seven years after the first examination (third row of images)
Clinical presentation: The patient hasn't been operated on, yet. She came to a repeat examination because of neck complaints, she felt pressure when lying down.
Palpation: a firm nodule in the left lobe.
Laboratory tests: TSH 1.70 mIU/L.
The dimensions of the nodule in the left lobe were 41x25x50 mm, width, depth, length, respectively, the volume of the lesion was 26.8 mL.
FNA resulted in follicular tumor.
Histopathology disclosed minimally invasive follicular cancer. The largest diameter was measured 55 mm. Both capsular and vascular invasions were found microscopically.
Comments. It is worth highlighting three changes. First, the nodule echogenicity has changed over time - from clearly hyperechoic to moderately hypoechoic. Secondly, the nodule substantially increased in size. This is the cause for the disappearance of the halo, due to the nodule growth, the capsule became invisible thin. Thirdly, the pattern of the intranodular hypoechoic parts has also changed.