
|
|
100 consecutive cases of papillary cancer - case 085
|
|









First examination (first row of images):
Clinical presentation: A 37-year-old man was referred for an evaluation of a 'lump in the throat' feeling.
Functional state: subclinical hypothyroidism with TSH 5.01 mIU/L, FT4 13.6 pM/L.
Palpation: the left lobe was suspicious containing a small nodule.
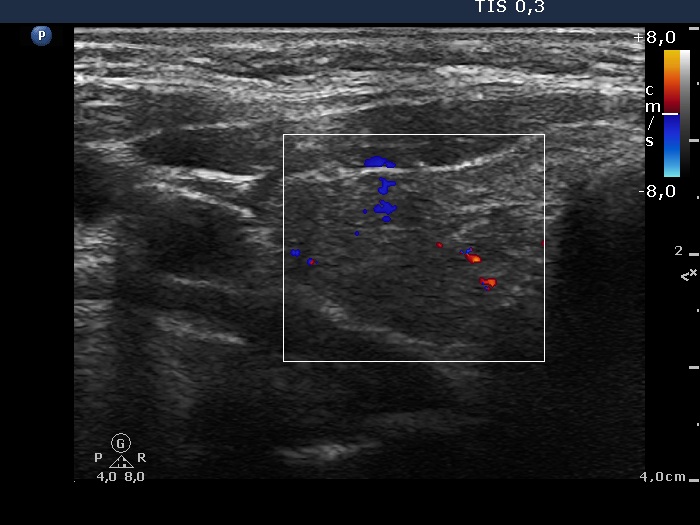
Ultrasonography. The thyroid was moderately hypoechogenic and displayed fibrosis. There was a relatively larger hypoechogenic lesion in the central part, and other smaller ones in the dorsal part of the left lobe. The dimensions of the largest lesion were 11x10x13 mm (width, depth, and length, respectively), the volume was 0.75 mL. The vascularization was not specific.
Aspiration cytology resulted in Hashimoto's thyroiditis. Atypia of unknown significance; the possibility of a Hürthle-cell tumor cannot be excluded.
We told the patient that the risk of malignancy is around 5%. We offered a follow-up examination instead of a surgery and suggested a repeat FNA in six months.
Second examination 7 years later (second row of images):
Clinical presentation. In the past 7 years, the patient had no complaints and therefore did not come to the proposed checkup either. Now he felt it was time to do an investigation.
Functional state: subclinical hypothyroidism with TSH 5.82 mIU/L, aTPO 98 U/mL.
Palpation: a hard nodule in the left lobe.
Ultrasonography. The presentation of the thyroid was essentially the same as 7 years ago. The only discrepancy was the lesion in the left lobe. Firstly, the size of the lesion have substantially increased to 25x18x25 mm (width, depth, and length, respectively), the volume was 5.89 mL which means that the volume became almost 8-times larger. Secondly, it was no more question whether the lesion was a pathological nodule or not. It turned out that this lesion is clearly a pathological nodule. Thirdly, in contrast to the former examination, the nodule has numerous microcalcifications and showed a clearly irregular, lobulated margins.
Aspiration cytology resulted in suspicion of papillary cancer.
Total thyroidectomy was performed, histopathology disclosed a T2 papillary cancer and Hashimoto's thyroiditis.
Comments:
We could not decide on the first ultrasound whether the lesion in the left lobe would be a nodule in a pathological sense. The presence of other similar areas decreased the possibility being the larger lesion a true nodule.
By reviewing the original smear, we found scattered numbers of grooves and two or three inclusions. It is difficult for a person to judge his or her own opinion, but it may well be that this pattern should not be judged as Bethesda III but as a suspicion of malignancy.