Halo sign and vascularization
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Differential diagnostics |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
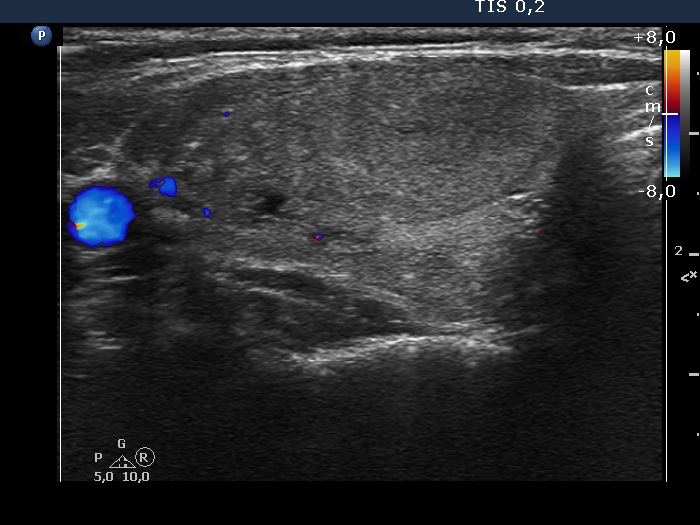
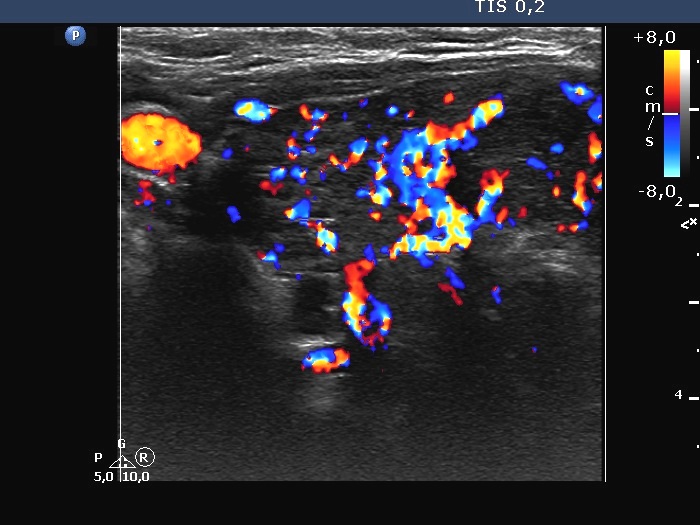
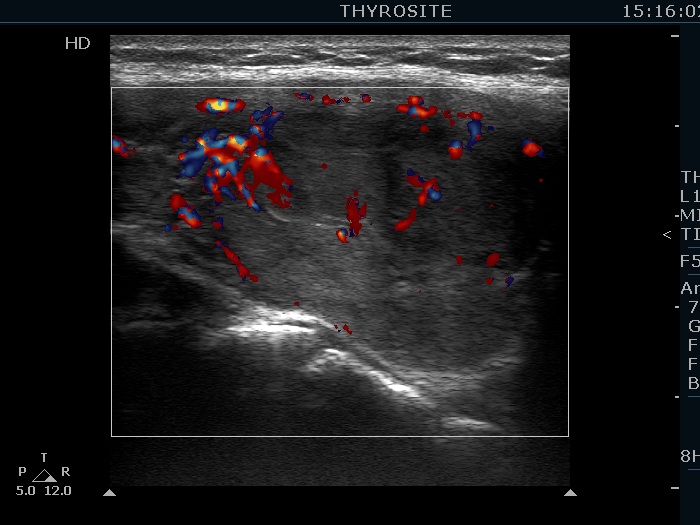
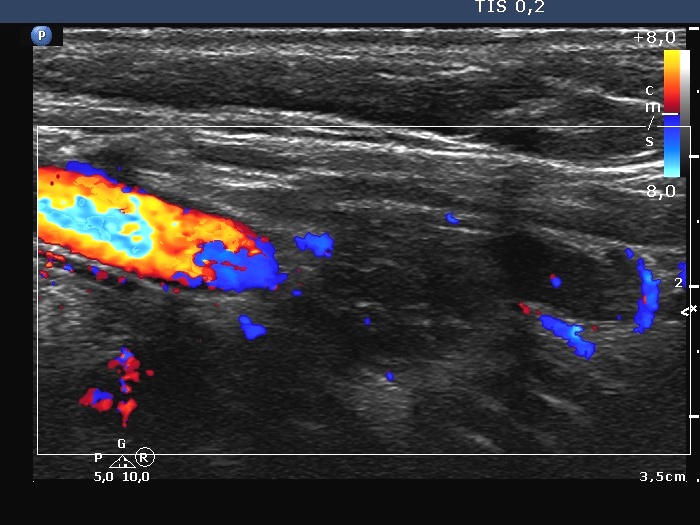
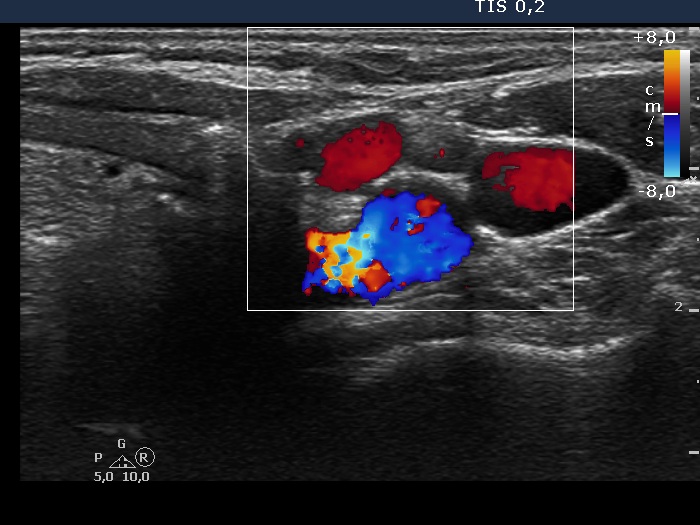
We demonstrate the various forms of vascular patterns in thyroid nodules. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Halo sign and vascularization
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 2. Differential diagnostics |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
We demonstrate the various forms of vascular patterns in thyroid nodules. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||