
|
|
The role of complex diagnosis - other examples - Case 2.
|
|



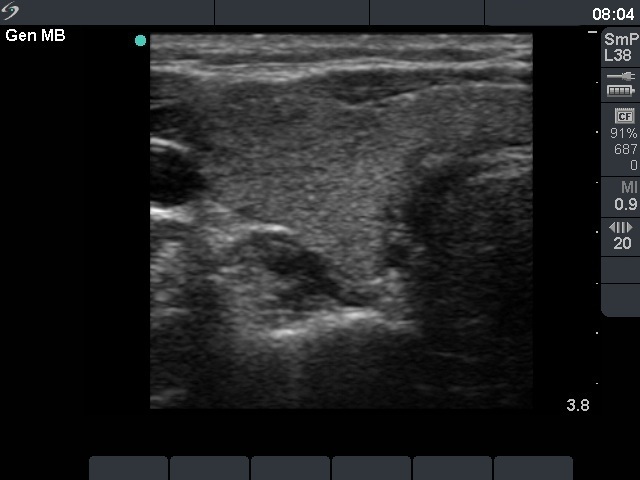




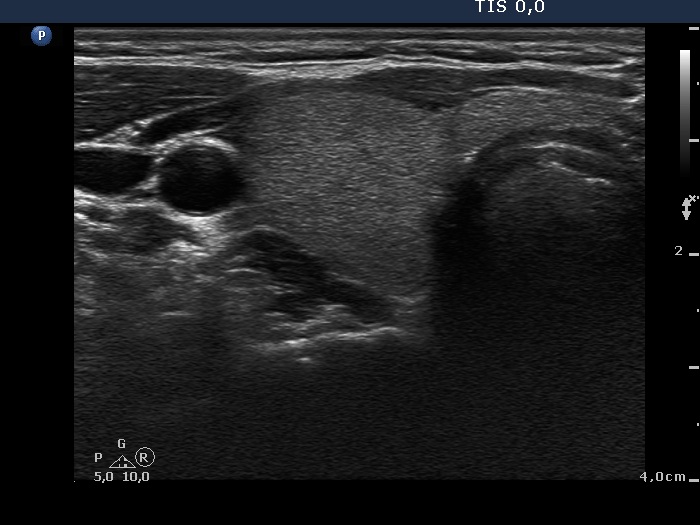


First examination (first row of images)
Clinical presentation: a 30-year old woman initiated a screening because her mother was operated on papillary thyroid carcinoma. The patient had no complaints. She was referred to me to an ultrasound examination.
Palpation: no abnormality.
Hormonal examination: indicated euthyroidism (TSH 1.93 mIU/L).
Ultrasonography: both lobes were partly echonormal partly minimally hypoechogenic. Small minimally-moderately hypoechogenic areas were present. There was no lesion of oncological significance. Our diagnosis was suspicion of autoimmune thyroiditis.
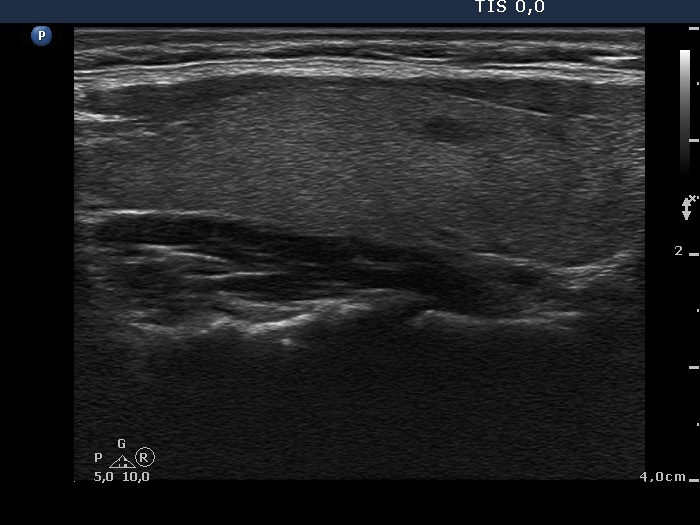
Second examination 14 months later (second row of images)
Clinical presentation: the patient visited us because she had two stillbirths, for a year and for seven months, respectively. After our ultrasound report her first evaluation was extended with an anti-TPO test which resulted in 0 U/mL, and the colleague's final report was "no thyroid abnormality". No thyroid examination was performed during her first pregnancy while an elevated TSH was detected on the 7th week of her second pregnancy (TSH 7.14 mIU/L) however she aborted his child the next day after the TSH test.
At present examination she was on 5th week of pregnancy. We asked the patient for the histopathological result of her mother which disclosed a T4N1 papillary carcinoma and a Hashimoto's thyroiditis.Palpation: no abnormality.
Ultrasonography: identical with the first examination.
Hormonal examination: subclinical hypothyroidism (TSH 5.98 mIU/L, FT4 12.2 pM/L) with a normal anti-TPO (0.5 U/mL).
We started a replacement therapy with daily 50 microgram levo-tiroxin.
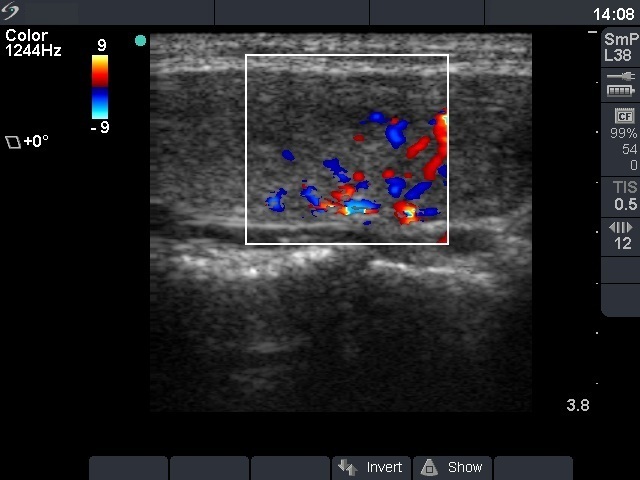
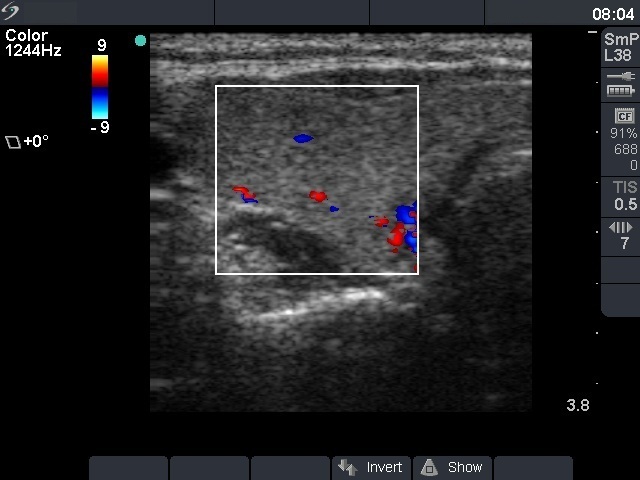
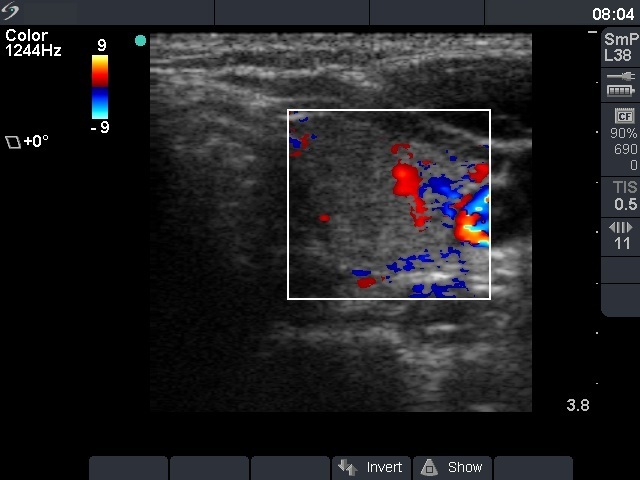
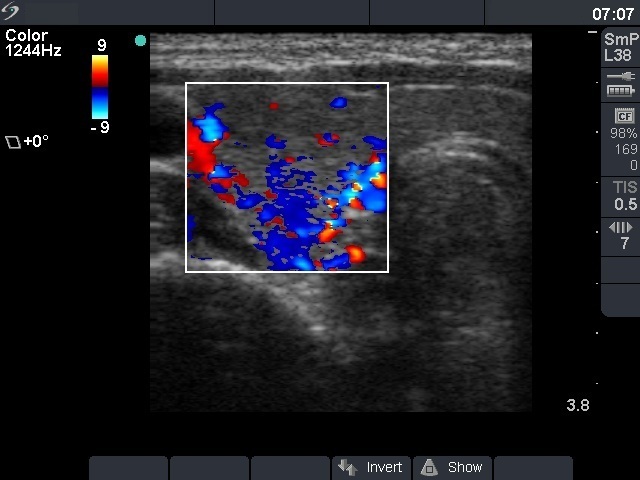
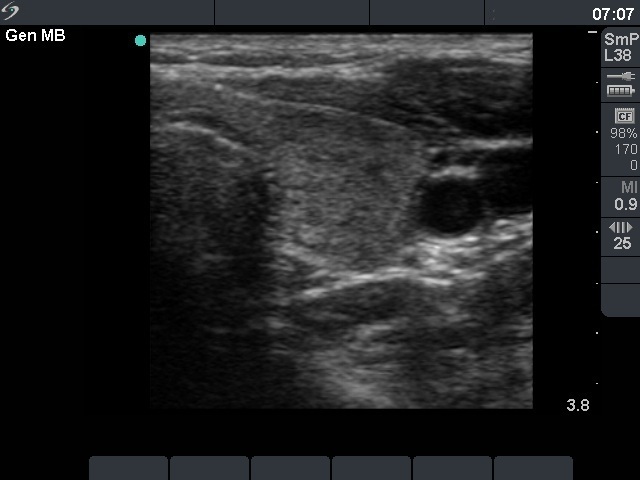
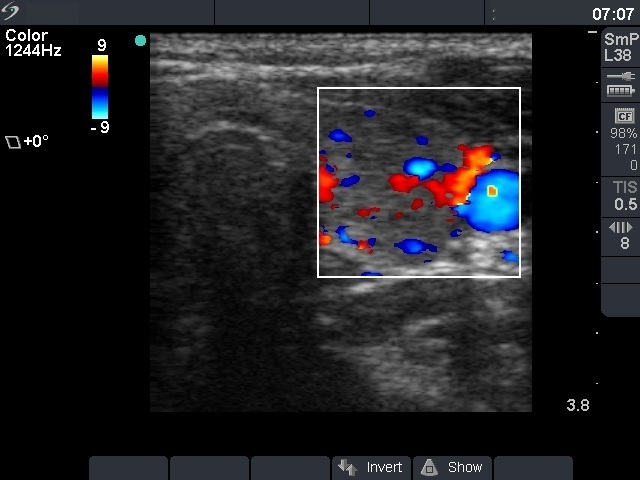
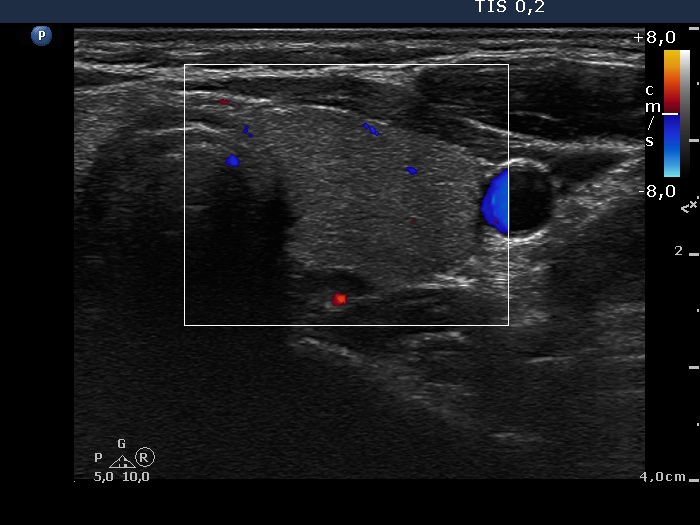
Third examination 25 months after first investigation (third row of images)
Clinical presentation: the patient delivered for 3 months. She had no complication neither during pregnancy nor during delivery. She was regularly checked during pregnancy and was on a daily 87.5 microgram levo-tiroxine at the time of delivery. Thereafter was suggested to leave the thyroid medication. She visited us now because of fatigue, hair loss and palpitation.
Palpation: no abnormality.
Ultrasonography: the thyroid became more hypoechogenic and the vascularization was increased.
Hormonal examination: subclinical hyperthyroidism (TSH 0.01 mIU/L, FT4 38.4 pM/L) with a normal TSAb (0 U/L) and an elevated normal anti-TPO (194 U/mL).
We did not administer any medication. (She wanted to continue with breast-feeding therefore beta-blocking agent was not given.)
Diagnosis: post partum thyroiditis.
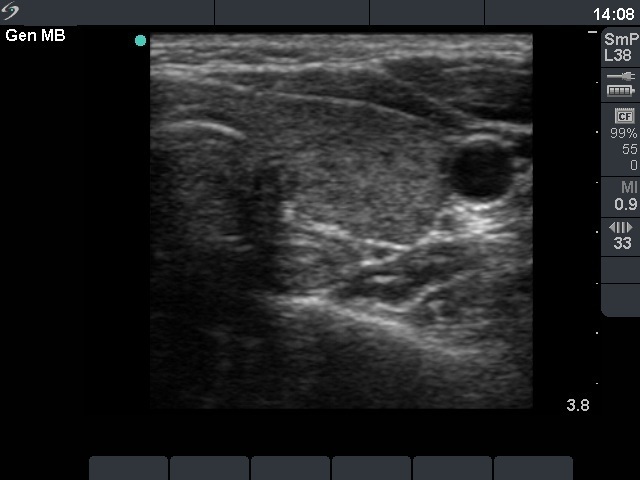
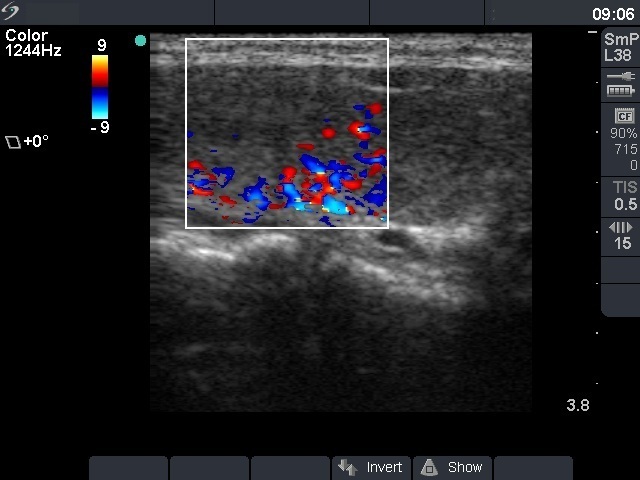
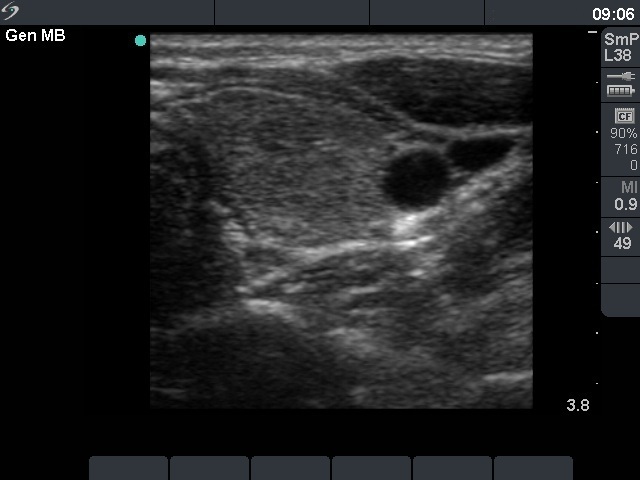
Fourth examination 31 months after first investigation, 8 months after delivery (fourth row of images)
Clinical presentation: except for fatigue the patient had no complaints. Three month earlier her thyroid tests were in the normal range (TSH 0.98 mIU/L, FT4 11.0 pM/L). She visited us now because of fatigue, hair loss and palpitation.
Palpation: no abnormality.
Ultrasonography: the thyroid was less hypoechogenic compared with the previous examination, the vascularization was already a bit increased.
Hormonal examination: mild degree of hypothyroidism (TSH 9.02 mIU/L, FT4 8.61 pM/L).
We did not give any medication.
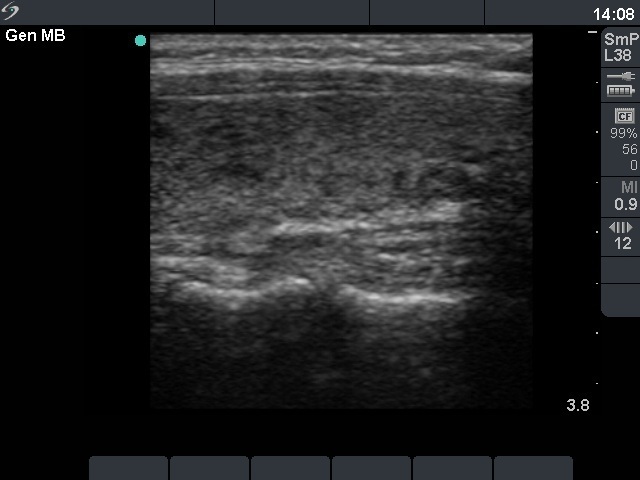
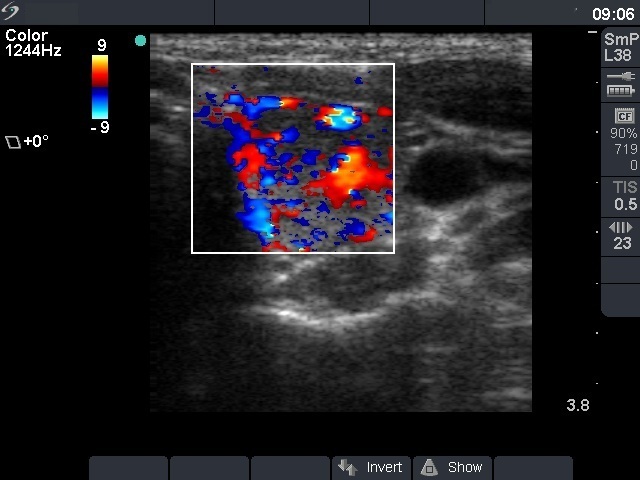
Fifth examination 58 months after first investigation (fifth row of images)
Summary of previous checking: 14 month after her delivery the thyroid became euthyroid and remained so. A regular thyroid checking TSH-test was prescribed with a TSH-test every year, in the event of pregnancy at once. The patient was now again pregnant at the 4th week of pregnancy.
Palpation: no abnormality.
Ultrasonography: the thyroid was almost echonormal and presented minimally hypoechogenic areas.
Hormonal examination: euthyroidism with a low TSH-level: TSH 0.07 mIU/L, FT4 19.4 pM/L.
We did not gave any medication. A repeat thyroid test was suggested in a month.
Comments.
-
Although there are conflicting results in the literature, even a mild degree of hypothyroidism might be associated with increased risk of stillbirth and miscarriage. Therefore at least those women who share an increased risk of developing a hypothyroidism should be regularly checked. On our opinion, the most important time point of checking is the early pregnancy within the first 5 week.
-
Ultrasound examination seems to be more sensitive detecting mild degree of an autoimmune thyroiditis than anti-TPO test. If the former suggest thyroiditis we advise regular TSH-checking. If the anti-TPO is normal, than every 2 to 3 years if the anti-TPO is elevated then every year, in both cases out of turn in early pregnancy.
-
There was another circumstance in this case which raised the suspicion of a higher risk for developing hypothyroidism. The histopathology of her mother's thyroid disclosed Hashimoto's thyroiditis. It increases the risk for developing hypothyroidism in her first degree relatives to 2.5-fold.
-
We initiate replacement therapy exclusively based on actual hormonal status because the thyroid status is not identical in each pregnancies. In this case least in two pregnancies the patient presented subclinical hypothyroidism while in a third pregnancy she did an almost opposite thyroid status.
-
It is worth to compare this case study with the following one.
.