
|
|
Secondary thyroid carcinomas - Case 15.Metastasis of a laryngeal adenoid cystic cancer
|
|











Clinical data: a 58-year-old man with hoarseness lasting for 3 weeks. Laryngology revealed palsy of the left recurrent nerve. The patient had chronic kidney failure and was hemodialyzed.
Palpation: the left lobe was enlarged but no nodule was palpable.
Functional state: euthyroidism with TSH-level 0.34 mIU/L, FT4 13.9 pM/L.
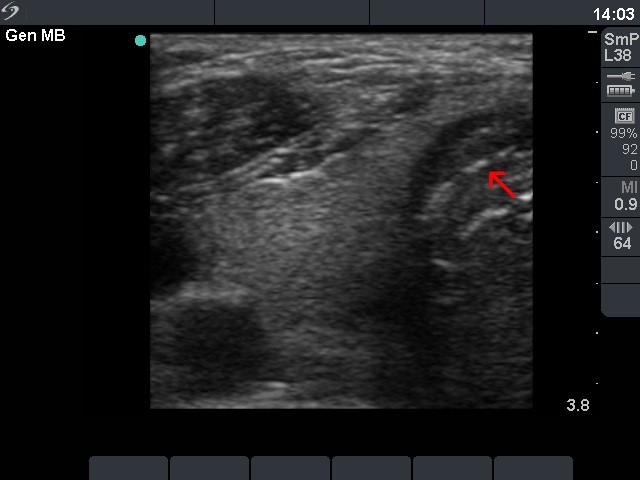
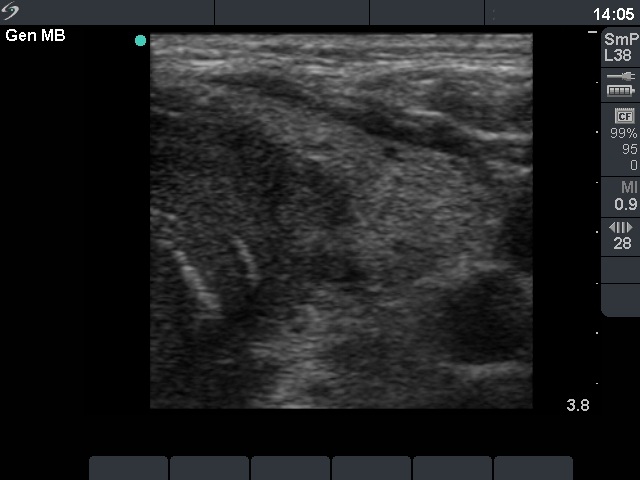
Ultrasonography: the right lobe was intact. On the dorsal part of the left lobe there was hypoechogenic mass spreading to the dorsal part of the isthmus. There was no blood flow within the nodule on color Doppler.
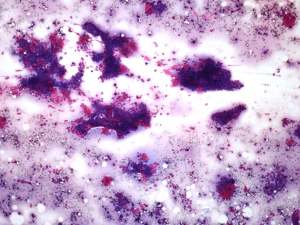
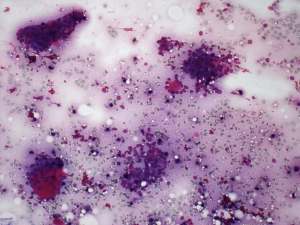
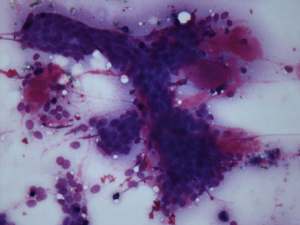
Cytology. Pictures of two smears are demonstrated. The presence of thick colloid is unusual in the case of a malignant tumor. Moreover, the cytological pattern highly resembles that of a papillary cancer.
Combined ultrasonographic-cytological diagnosis: carcinoma. The possibility of a papillary, that of a medullary cancer and even a metastasis should be considered.
Blood test for calcitonin: serum-level of calcitonin exceeded 706 pg/mL (normal value < 10).
Our final diagnosis was medullary carcinoma.
A total thyroidectomy was performed. Histopathology: metastasis of an adenoid cystic carcinoma of unknown origin.
On postoperative evaluation a laryngeal adenocancer was found as the primary focus of the cancer. This is a very rare tumor of the larynx which accounts less than 1% of laryngeal carcinomas. For a case report click here . Three months after surgical removal of the whole thyroid the cacitonin test was negative.
Comments:
-
The US pattern is very specific for cancer. Such macroscopic proof of an invasively spreading cancer is rarely seen. The lack of enlarged lymph nodes in the neck would be a very unusual finding in the event of such an aggressive form of a papillary or medullary cancer. This property itself raises the possibility that the thyroid carcinoma is not a primary one.
-
We had two false positive calcitonin reactions between 1991-2012. This was the only case with IRMA method. Increased calcitonin levels have been described in cases of chronic kidney failure and in hemodialyzed patients (in up to 25% of the latter patients).
-
If we took two independent features into account, i.e. the lack of lymph node metastasis in such an aggressive tumor and the possibility that the calcitonin test can be false positive we could avoid the false diagnosis of medullary carcinoma.
-
The cytologic picture itself was very deceptive, distinct part of the smears mimicked three distinct thyroid entities, a colloid goiter, a papillary cancer and a lymphocytic thyroiditis. The presence of solid nests and that of metachromatic material may be the clue of avoiding false diagnosis of a primary thyroid lesion of follicular cell origin. Nevertheless, the cytopathologist would be in a very difficult situation if he or she would not be aware of clinical and sonographic details.