
|
|
Chronic lymphocytic thyroiditis - Case 72.
|
|

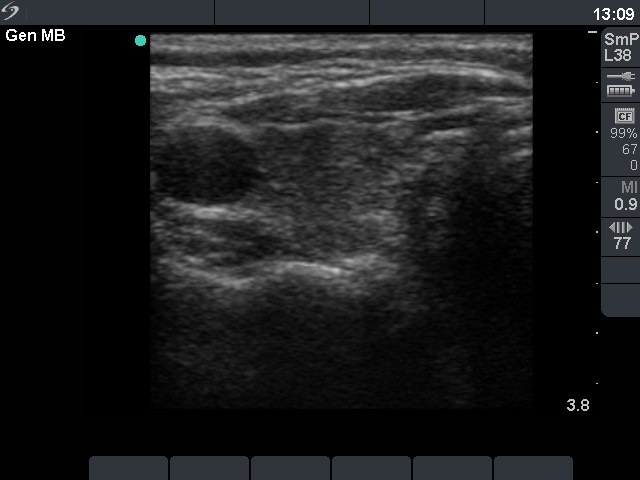
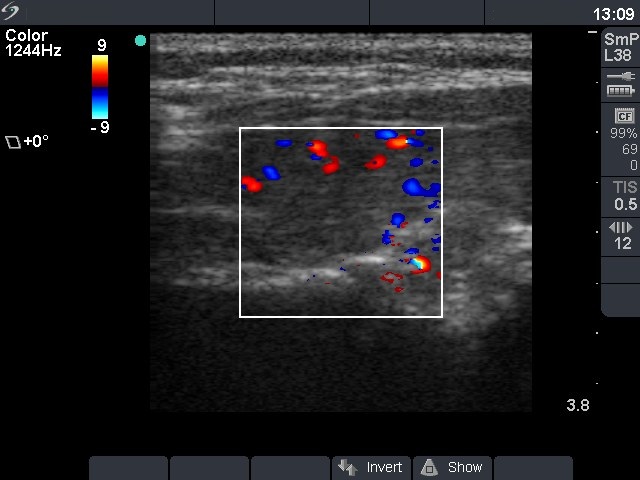


Initial examination (first row):
Clinical presentation: a 50-year-old woman was referred for an evaluation of a low TSH-level detected on a routine examination because of gastorintestinal complaints and 7 kg loss of weight.
Palpation: no abnormality.
Functional state: mild hyperthyroidism with TSH 0.02 mIU/L, FT4 38.1 pM/L, FT3 7.99 pM/L.
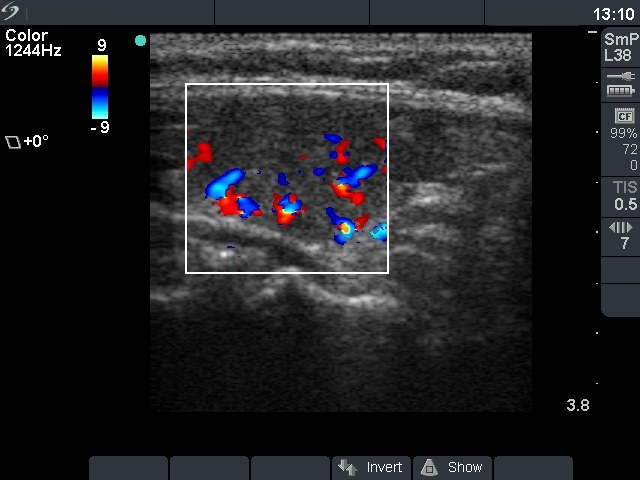
Ultrasonography: the thyroid was moderately hypoechogenic without any nodule. The vascularization was increased but not to the degree which was usually observed in Graves' disease.We performed TSH-receptor antibody test which yielded normal result 0 U/L, and anti-TPO determination which resulted in 779 U/mL.
Clinical diagnosis: hashitoxicosis.
We administered beta-blocking agent and advised a repeated examination 2 months later.
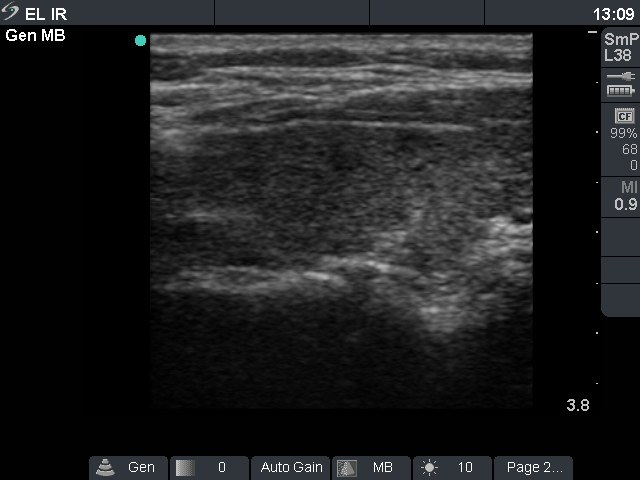
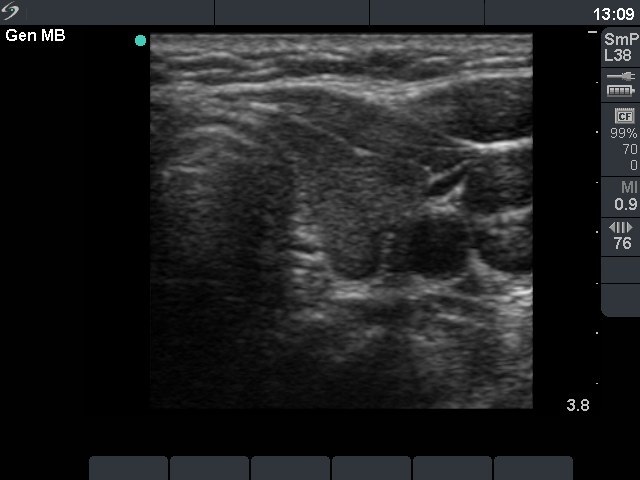
Second examination 4 months later (second row):
Clinical presentation: the patient has regained the weight loss. She was fatigue and had hair loss.
Palpation: no abnormality.
Functional state: hypothyroidism with TSH-level 0.12 mIU/L, FT4 8.07 pM/L. The seeming contradiction between the low TSH and low FT4 level is explained by the difference in period which is measured by the two methods, and the relatively long recovery time of low TSH. The TSH reflects a longer period, while FT4 is a much shorter one, around 3 months and 2-3 weeks, respectively.
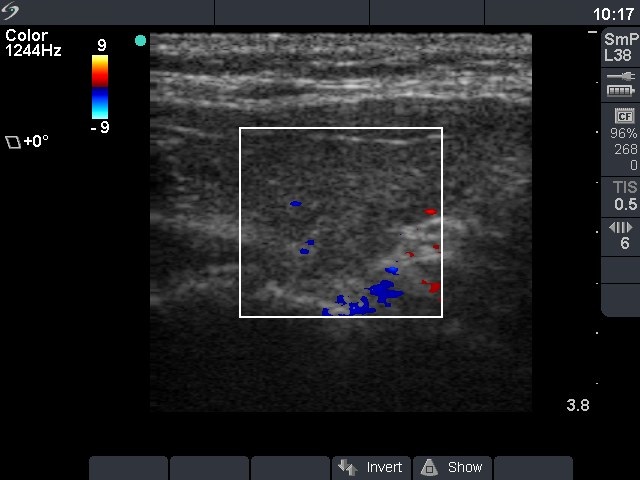
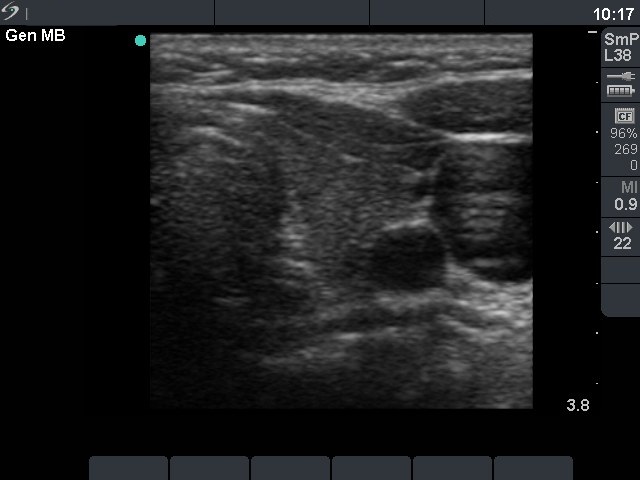
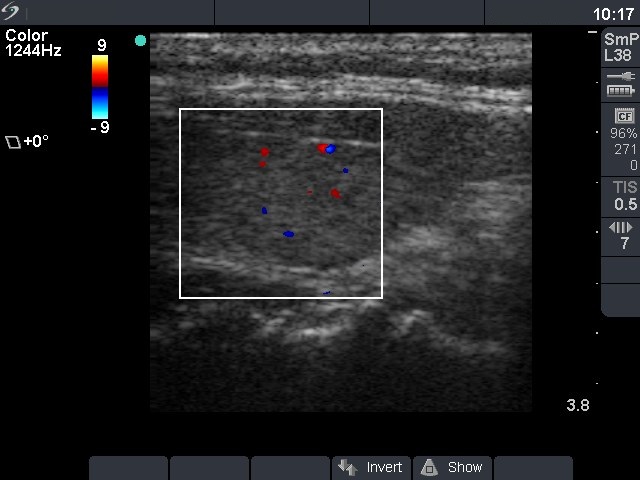
Ultrasonography: the vascularization decreased over time. Otherwise the ultrasound pattern was almost identical with the previous one.
6 months later the patient became clinically and biochemically euthyroid. A yearly TSH determination was suggested.