
|
|
The role of complex diagnosis - follow-up of follicular lesions - Case 6.
|
|

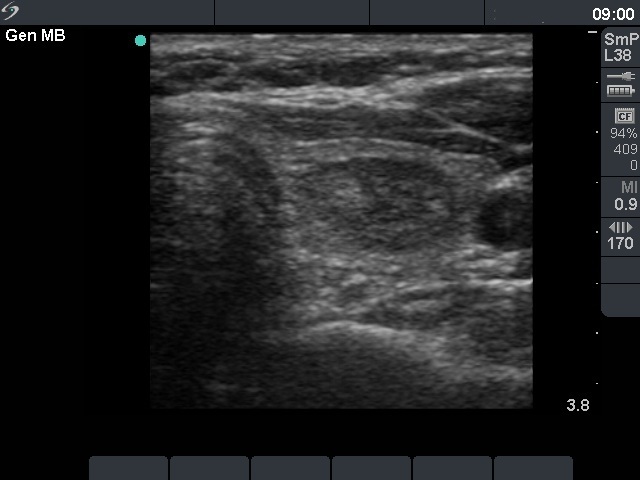
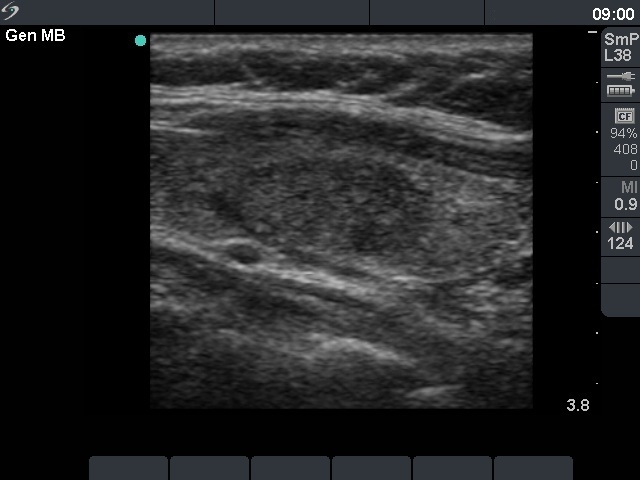



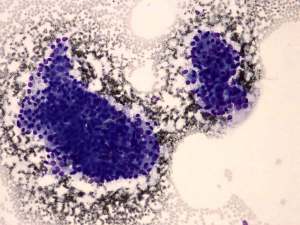
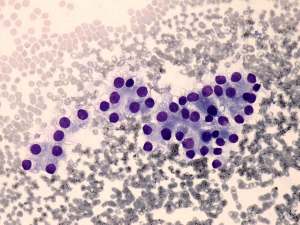
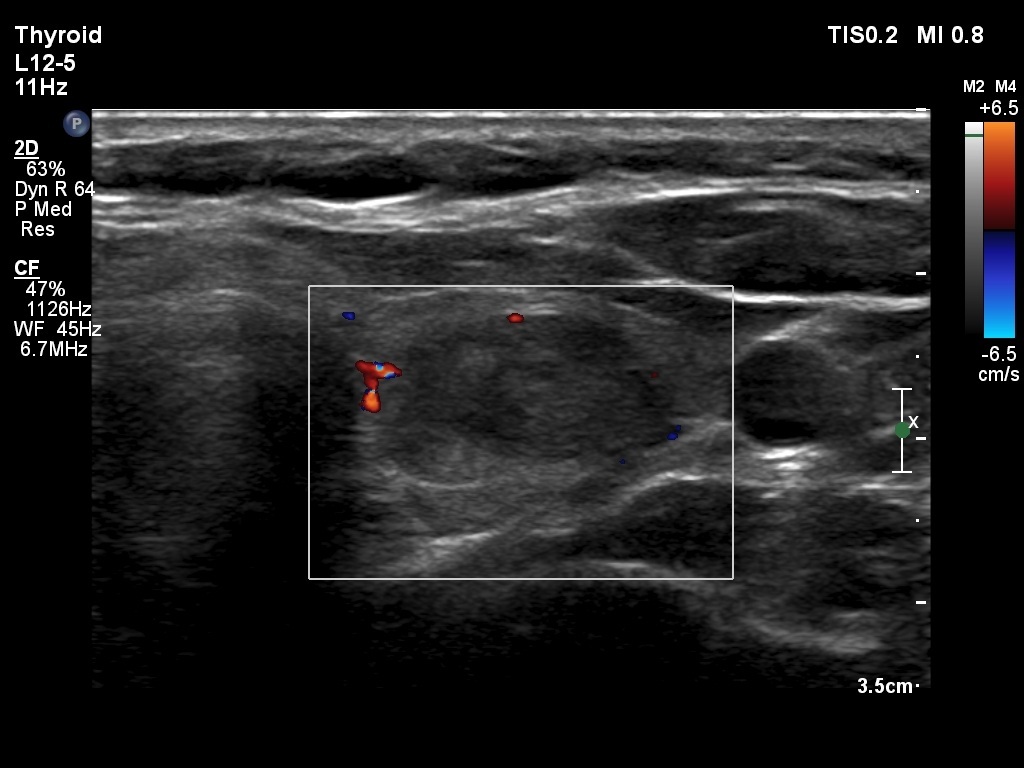
First examination (1st and 2nd rows of images)
Clinical presentation: a 45-year-old woman was referred for evaluation of a nodule discovered by carotid Doppler examination.
Palpation: a not firm nodule in the left lobe.
Functional state: euthyroidism with TSH-level 1.33 mIU/L.
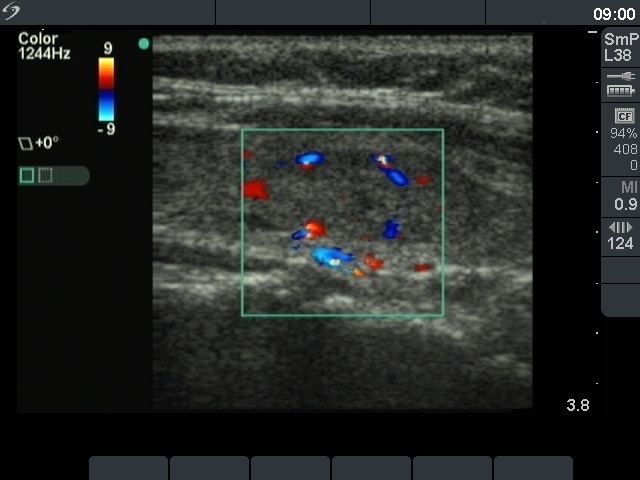
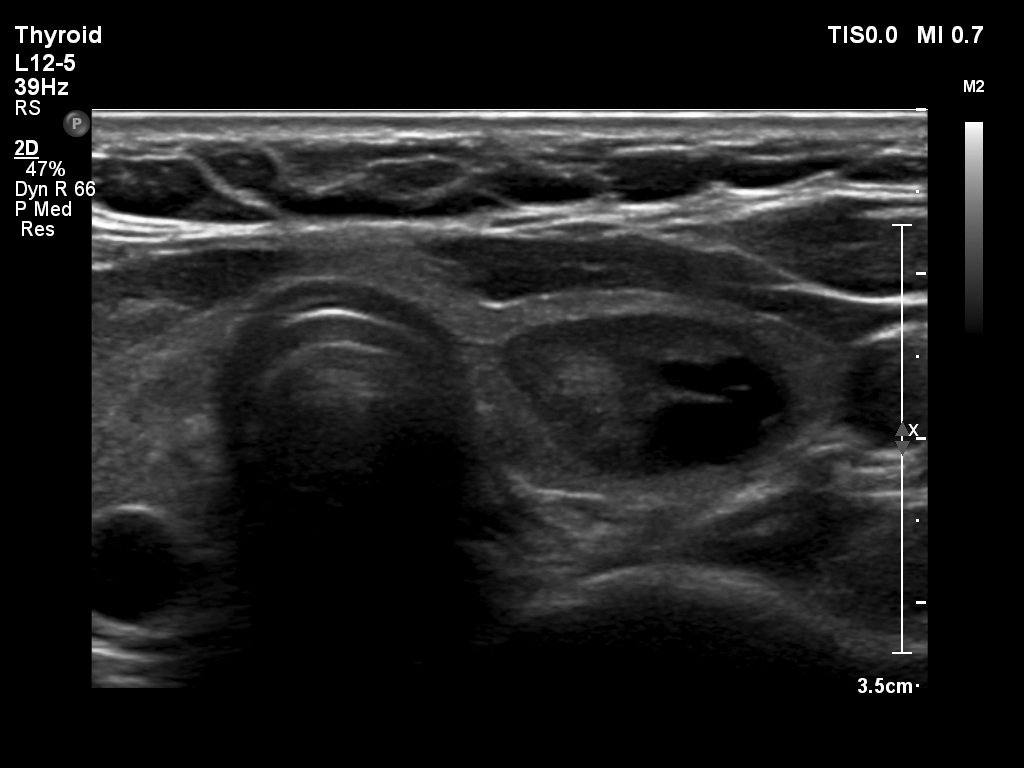
Ultrasonography. The thyroid was echonormal. There was a moderately hypoechogenic, inhomogeneous nodule in the part of the left lobe. The nodule presented a type 3 vascular pattern.
Cytological pattern corresponded to a follicular tumor without significant atypia.
A combined clinical-ultrasound-cytological diagnosis was benign follicular proliferation with less than 1% risk of carcinoma.
We advised regular follow-up instead of immediate surgery.
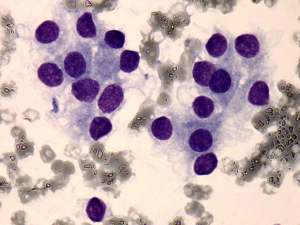
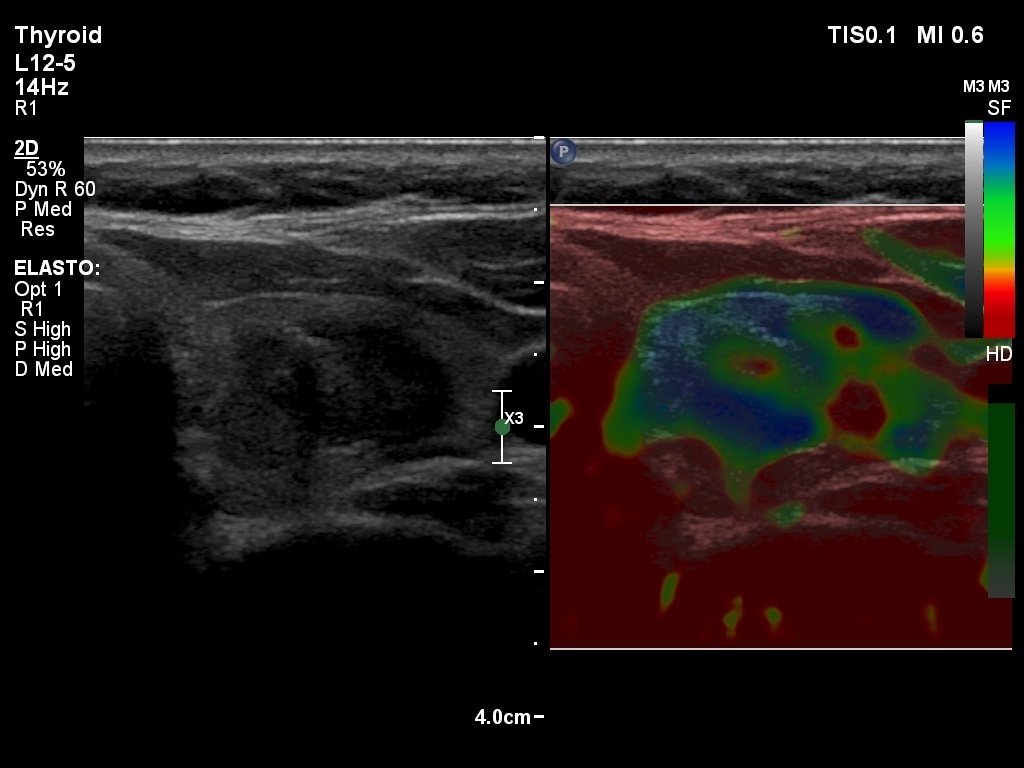
Second examination 2 years later (3rd row of images)
Summary of follow-up: the patient had no complaints.
Functional state: euthyroidism with TSH-level 1.76 mIU/L.
Ultrasonography: the ultrasound presentation of the thyroid was basically unchanged except for the presence of cystic area within the nodule. The vascularization and elastography of the nodule were not specific.
Suggestion: to continue the follow-up with ultrasound and TSH determinations every three years.
Comment. the presence of a halo and a perinodular blood flow significantly increases the possibility of a follicular tumor with the likelihood of around 50%. Nevertheless, great proportion of hyperplastic nodules also exhibit these ultrasound signs. On the other hand, the absence of both a halo and a perinodular blood flow not simply decreases the likelihood of a follicular tumor but makes this possibility very unlikely: less than 2% of such nodules proves to be follicular tumors.