
|
|
Chronic lymphocytic thyroiditis - Case 17.
|
|





Clinical presentation: a 55-year-old woman was treated for hyperthyroidism for 13 years. She visited her endocrinologist because of her diffuse complaints including 3 kg gain in weight, fatigue and hair loss. A multinodular goiter was found on the examination. Aspiration cytology resulted in suspicion of follicular carcinoma. Total thyroidectomy was planned. The patient requested a second opinion.
Palpation: both thyroids were firm and nodular on palpation.
Functional state: euthyroidism (TSH 2.06 mIU/L, TSAb negative, aTPO 9 U/mL).
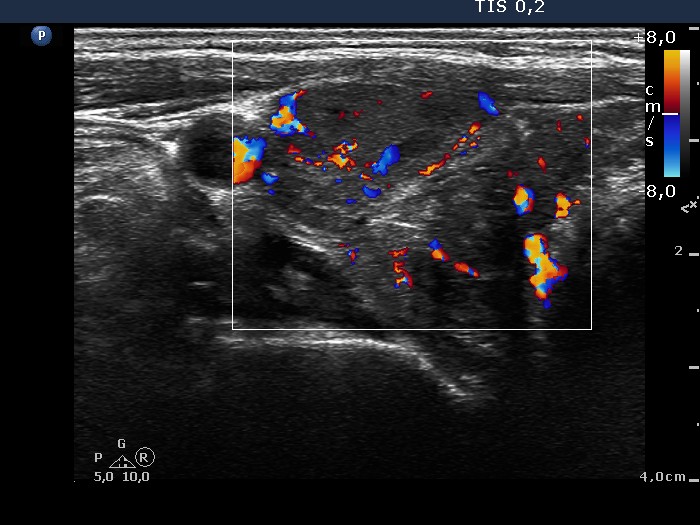
Ultrasonography: the basic echo structure of the thyroid was moderately hypoechogenic. There were many discrete lesions with various echo patterns. The lesion in question was located in the left thyroid. It was hypoechogenic, inhomogeneous, presented coarse calcification and displayed neither a halo sign nor perinodular blood flow.
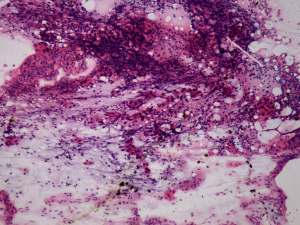
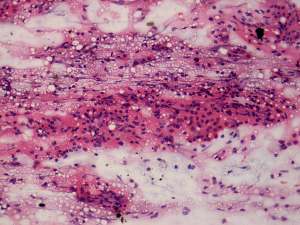
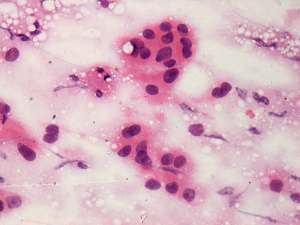
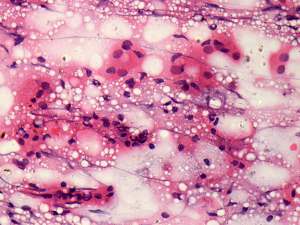
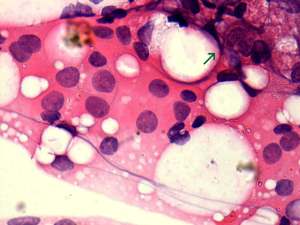
Cytology: was performed from a hypoechogenic area in the right lobe and from the lesion from which the FNAC was suspicious on previous examination. In both cases the diagnosis was Hashimoto's thyroiditis.
Histopathology: disclosed Hashimoto's thyroiditis without any nodule. A coarse calcification was found in the left thyroid.
Comments.
-
Most follicular tumors present a halo sign and/or perinodular blood flow. The lack of both of these properties significantly decreases the chance of a follicular tumor.
-
Despite the normal antibody levels, the basic ultrasound pattern itself was suspicious for autoimmune thyroiditis.
-
Although except for rare special instances a positive cytology decides that the patient has to be operated, a repeated cytology may be important if we have any doubt about the initial cytological result. This patient could avoid an unnecessary bilateral thyroidectomy. Hashimoto's thyroiditis may cause the greatest concern in thyroidology. Both the cytological and the ultrasonographic patterns may be extremely various.